
The Centers for Medicare and Medicaid Services’ (CMS’) Electronic Health Record (EHR) Incentive Program—Meaningful Use—requires that eligible providers participating in the incentive program successfully demonstrate meaningful use of the EHR system by reporting on a set of core and menu functional objectives to qualify for incentive payments of up to $44,000.
If you want to earn the incentive payment, it is imperative to review and fully understand the objectives as well as how and in what form the objectives are measured. Simply reviewing a list of Meaningful Use objectives and then working from there will not lead to success. The devil is in the details of what really needs to be done to meet those objectives. Work with your EHR vendor to verify that the appropriate processes for data entry are in place so that your EHR system can measure and report in a way that truly meets the measure and proves to CMS that you are a meaningful user of the EHR.
Understanding the Measures
Each of the Stage 1 objectives for Meaningful Use has an associated measure to gauge compliance and guide reporting (see Figure 1, right, and Figure 2 p. 20). These measures include specific terminology that clarifies how the objectives will be measured and the threshold that you must meet to be considered successful and qualify for incentive payments.

Among these is the concept of a “unique” patient. Many measures are based on counting data entered into the EHR or actions taken based on unique patients. A unique patient is one that is seen by the eligible provider more than once during the EHR reporting period. When a measure is based on unique patients, for the purposes of measurement calculation, that patient is only counted once in the denominator population for the measure regardless of the number of visits that patient had during the reporting period. For example, when the calculation in your first payment year (reporting year refers to the first year the eligible professional [EP] submits for payment, regardless of the calendar year, and is a 90-day period) is performed for the computerized physician order entry objective, the EHR system will review all the patients whom you have seen at least twice during that 90-day period and will count each patient, not each visit, once.
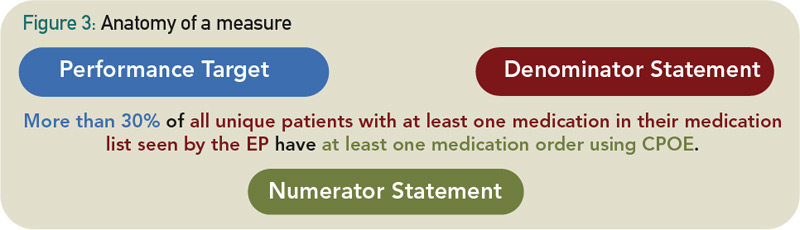
Each measure will be assessed and reported based on a percentage or a yes/no attestation. Many of the core objectives require measures reported according to a specified numerator, denominator, and exclusions (if relevant). The denominator identifies all the eligible cases for a measure, and the numerator describes an outcome or action relevant to that denominator population—most often the number of activities or functions performed using an EHR (see Figure 3, below right).
For the Meaningful Use Objectives, the denominator is based on one of the following:
Simply reviewing a list of meaningful-use objectives and then working from there will not lead to success.
- Counting actions for patients whose records are maintained using certified EHR technology.
- Example measure: More than 40% of all permissible prescriptions written by the EP are transmitted electronically using certified EHR technology.
- What this means: The denominator includes all patients whose records are maintained in the certified EHR system. Other patients seen by the eligible provider but not recorded in the EHR (e.g., those with paper records) are not included in the denominator. For this measure, the denominator would include all of the permissible prescriptions, excluding controlled substances, for patients whose records are in the EHR system. The numerator would then identify how many of those prescriptions were generated and sent via electronic prescribing.
- All unique patients seen during the reporting period, regardless of whether the patient’s records are maintained using certified EHR technology.
- Example measure: More than 50% of all unique patients seen by the EP have demographics recorded as structured data.
- What this means: The denominator includes all unique patients seen during the reporting period, including those with both paper and electronic documentation. The eligible provider will need to generate a report of patient records stored in the EHR and also manually count any paper records for unique patients seen during the reporting period. The numerator would then assess how many of those patients have demographics entered into the EHR system as structured data.
- Count of actions for qualifying unique patients whose records are maintained in the certified EHR technology.
- Example measure: More than 30% of all unique patients with at least one medication in their medication list seen by the EP have at least one medication order entered using the computerized physician order entry (CPOE).
- What this means: This denominator refines “counting action” denominators, including only unique patients who meet additional criteria (e.g., a specified event). In this measure, the denominator includes all patients seen more than once by the EP and who have at least one medication in their medication list. The numerator would then assess how many of those patients had at least one medication entered via CPOE.

For those objectives that aren’t quantified using a percentage and performance threshold, the rule calls for reporting via yes/no attestation.
EPs Practicing in Multiple Locations
For those EPs practicing in multiple locations with certified EHR technology available for 50% or more of their total patient encounters during the reporting period, EHR reporting for Meaningful Use will only include those encounters where certified EHR systems are available at the start of the reporting period.
For example, the objective calling for more than 80% of all unique patients seen by the EP have at least one problem list entry or an indication that no problems are known for the patient recorded as structured data. Therefore, if an EP only practices at one location or has certified EHR technology available at each one of his practice locations, then the denominator would be all unique patients seen during the EHR reporting period, regardless of the location. However, if the EP practices at multiple locations and only has certified EHR technology available at two of his three practice locations—totaling 80% of his patient encounters during the reporting period— then the denominator population is only those unique patients seen at locations where certified EHR technology is available. This means that the EP will need to review the measures based on the collective total of unique encounters for all of the practice sites where certified EHR technology is available at the start of the reporting period.
Reporting Period
Note that Meaningful Use measures are limited to a period of time equivalent to the reporting period, meaning that the “count” will start on the date at which you intend to begin reporting and end on the date at which the reporting period ends. A period of 90 days is required for the first year that an EP begins reporting on Meaningful Use, and a full calendar year for each reporting year thereafter.
The 90-day reporting period that is required for the first year may lessen the burden associated with the initial reporting and program learning curve. Keep in mind, however, that the shorter reporting period also reduces the number of patients in the measure denominator, making it critical to track your progress and act on each opportunity to satisfy the Meaningful Use objective.
Understanding the CMS EHR Incentive Program requirements is no easy feat. The ACR is here to help! Visit www.rheumatology.org/HIT for more information and resources to help your practice meet the measure and achieve meaningful use. Also, be sure to read “Behind the Digital Door” on p. 52 of this issue to learn more about rheumatology practices that are working to become meaningful users.