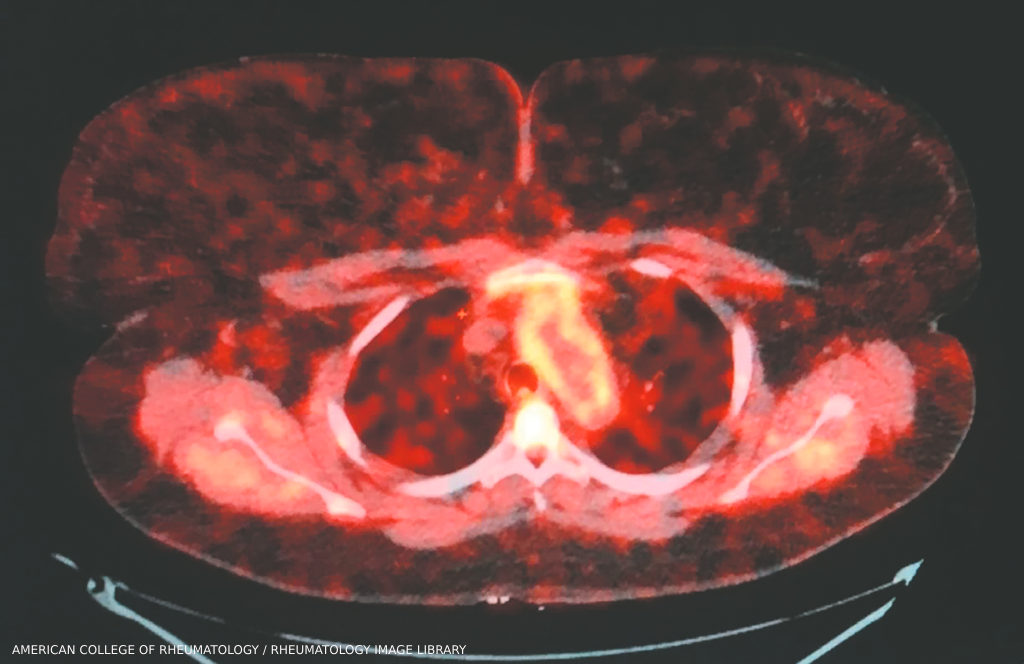
Takayasu arteritis: Aortic root enhancement on a PET-CT scan. A 30-year-old woman with long-standing Takayasu arteritis on infliximab and methotrexate developed chest pain and left arm claudication. PET scan showed 18-fluorodeoxyglucose avidity of the wall of the aortic root and arch indicative of active aortitis. (Click to enlarge.)
The rare systemic inflammatory disease known as Takayasu arteritis primarily targets the aorta and its major branches, such as the carotid arteries that direct oxygenated blood to the brain. Chronic inflammation of the arteries can yield complications, such as aneurysms and stenosis, or a narrowing and blocking of blood vessels that can prevent parts of the body from receiving enough blood and oxygen. This ischemia can lead to tissue damage.
Researchers remain in the dark about the underlying cause of Takayasu arteritis, adding to the challenges of identifying and managing the disease. “We still don’t understand, for example, how much genetics, relative to non-genetic factors, contribute to the disease etiology,” says Amr H. Sawalha, MD, chair of the Department of Pediatric Rheumatology and director of the Comprehensive Lupus Center of Excellence at the University of Pittsburgh Medical Center.

