Overlapping Myositis
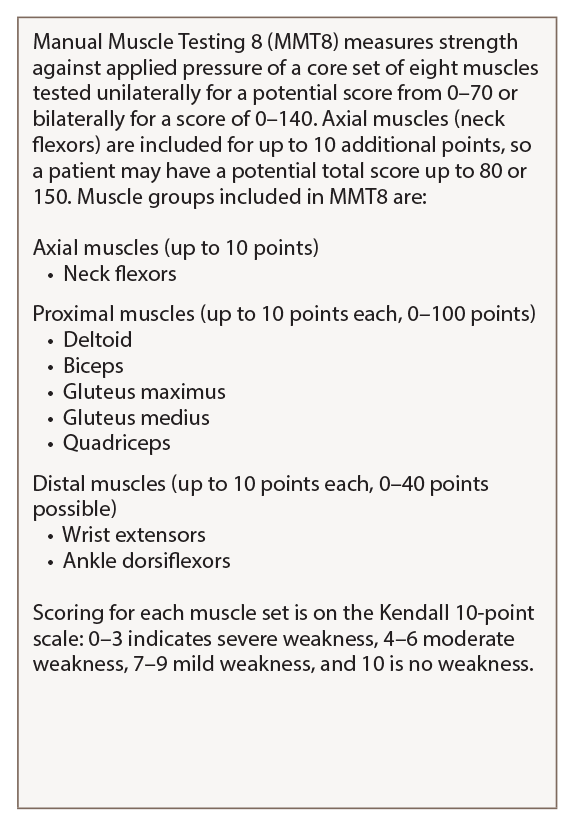
Table 1: MMT8
For a detailed guide on how to perform and score the MMT8, see Manual Muscle Testing Procedures for MMT8 Testing from the National Institute of Environmental Health Sciences.
Myositis may overlap with other rheumatic diseases, most often systemic sclerosis (SSc), but also rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE), said Julie J. Paik, MD, MHS, assistant professor of medicine, Johns Hopkins Scleroderma Center and Johns Hopkins Myositis Center.
Researchers have attempted to describe and classify patients with overlap myositis (OM) conditions. A 2005 study found that up to 29% of subjects in a Canadian myositis cohort had an overlap syndrome.9 A 2014 study found that 23% of myositis patients in a Brazilian cohort had overlapping RA and 29% had overlapping SLE, she said.10 “This may include myositis with a few overlapping connective tissue disease features, such as Raynaud’s phenomenon, arthritis, ILD, and a few features of SSc and lupus,” or on the other hand, patients met strict criteria for both myositis and the overlapping condition such as scleroderma, she said.

