The cardiologists’ suggestion that high-dose aspirin be administered alone as first-line therapy for patients with pain and arthritis might have been true as a recommendation 40 years ago, but I would venture to say that there are few—if any—rheumatologists today who use full doses of aspirin as primary therapy for osteoarthritis.
Source:
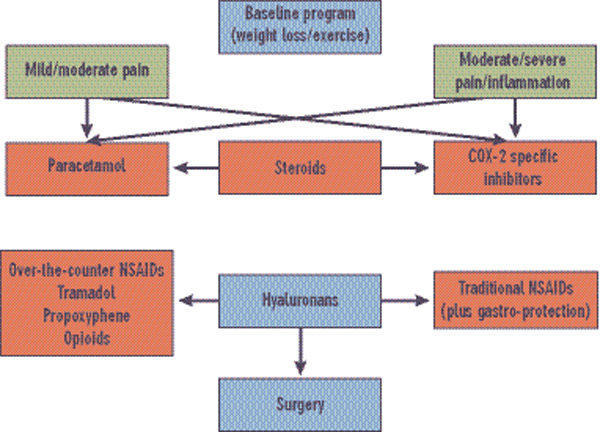
ACR Subcommittee on OA Guidelines.
Arthritis Rheum. 2000; 43:1905-1915.
With respect to guidelines for treating OA, the importance of risk versus benefit is, without question, always an uppermost consideration. Unfortunately, pain itself is a cardiovascular risk factor related to increased blood pressure and pulse rate, so lack of pain relief can put the patient at increased risk. Treatment paralysis is not an attractive alternative. Risks of any type are not to be considered lightly, and need to be balanced against relief of pain and improved quality of life—not always an easy decision. Judgment calls by both the patient and physician are important in determining eventual management in any given individual.

