Visit www.rheumatology.org/practice, and click on “Office Support” for PQRI coding instructions and a complete list of applicable codes for the rheumatology practice.
Registry
As an alternative to claims-based reporting, a provider may participate in an approved registry, which will submit PQRI quality-measure results and numerator/denominator data to CMS on the provider’s behalf. Registry reporting eliminates the need to submit CPT II codes through claims. A list of qualified registries for 2010 PQRI can be found on the CMS PQRI Web page titled, “Qualified Registries for 2010 PQRI Reporting.”
There are several benefits of reporting via registry.
- First and foremost, the success rate for registry reporting is generally much higher than claims reporting—the success rate in 2008 was 96%.
- Registries provide data quality checks to ensure that all submissions are accurate and complete to avoid rejected measurements.
- The ability to enter and view this data at any point throughout the reporting year means that data entry or chart review can be performed retrospectively in a batch format.
- Most registries will allow you to submit your 2010 data right up until the CMS deadline in late February 2011, eliminating the need to track claims throughout the year. If it’s decided late in 2010 to report PQRI data for the past year, it can be done through a registry. This is not so with claims-based reporting.
- Finally, registries often provide more timely access to data and analyzed reports, which can contribute significantly to practice improvement efforts.
The ACR’s clinical quality registry, the Rheumatology Clinical Registry (RCR), is approved by CMS for PQRI reporting. Through the RCR, ACR members and their staff can submit quality data on the RA measures group for the required 30 patients. For more information on the RCR, visit www.rheumatology.org/rcr.
Measures to Be Reported
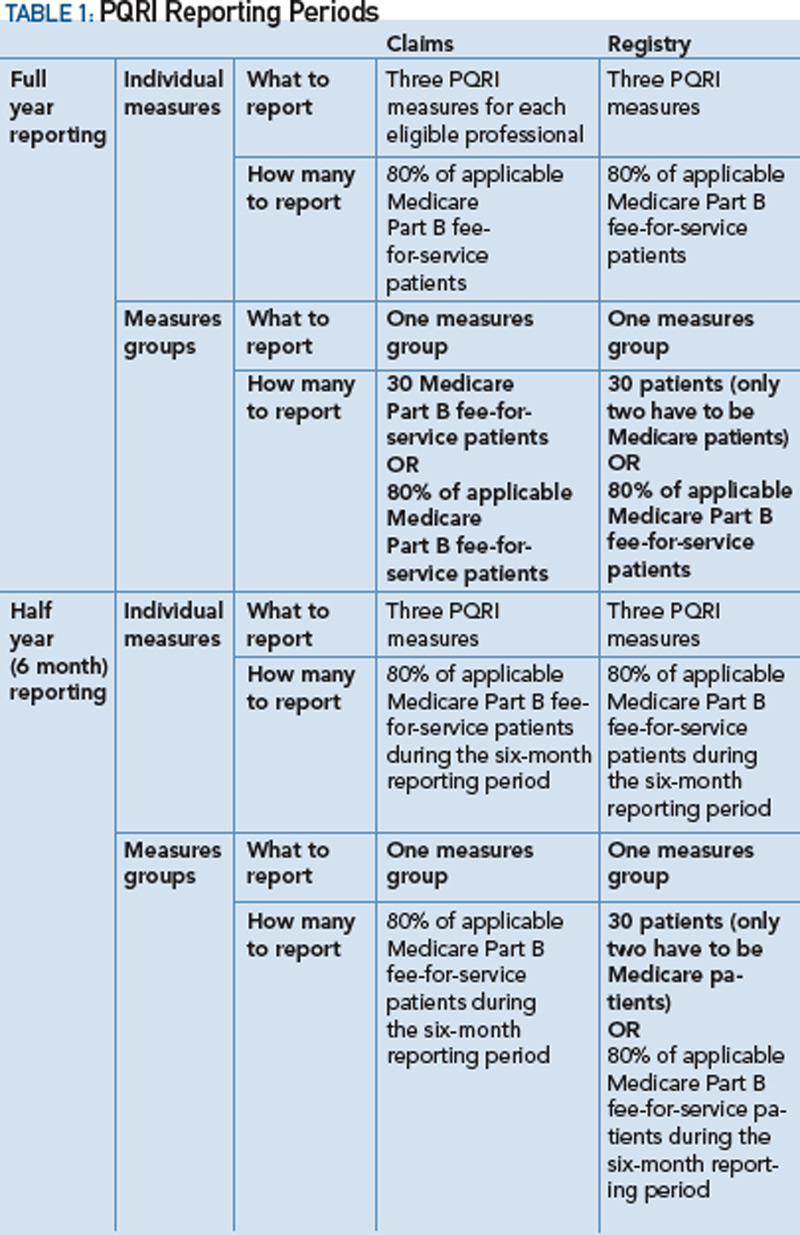
Providers can choose to report on either three individual measures or a single measures group.
