click for large version
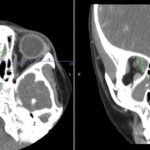
Axial (left panel) and sagittal reformat (right panel) contrast enhanced CT scan of the orbit showing tumefactive mildly enhanced perineural soft tissue density encasing right optic nerve, involving retroconal space (red circle) and extending to lateral and superior recti muscles (blue circle) consistent with orbital pseudotumour. Another left side perineural small nodule is also seen (arrow).
Discussion
The eye is frequently involved in SLE, with the most common manifestation being keratoconjunctivitis sicca. Other less common causes include cotton wool exudates due to retinal vasculitis, episcleritis and scleritis.