Click here to view abstract video
Click here to view abstract video Click here to view visual abstract summary
Click here to view visual abstract summary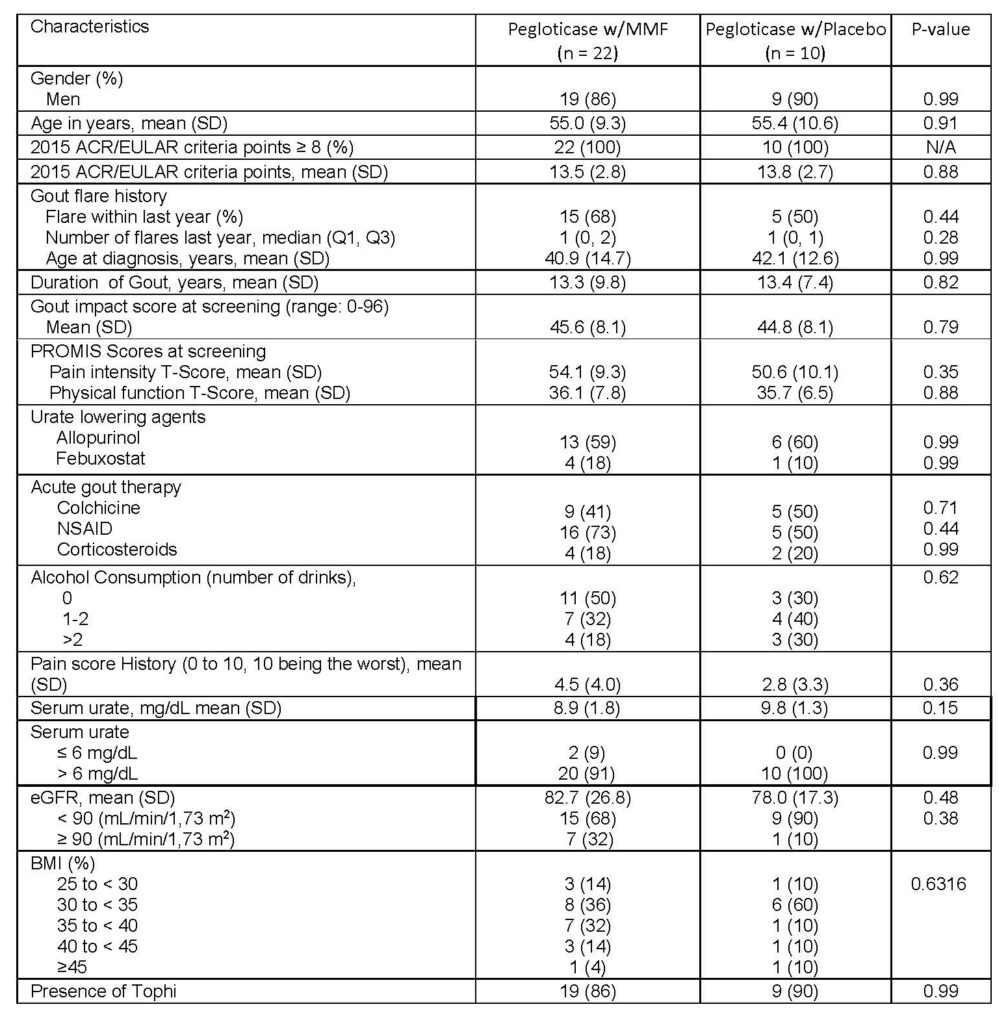
Table 1. Patient demographics for treatment arms of pegloticase with MMF and pegloticase with placebo
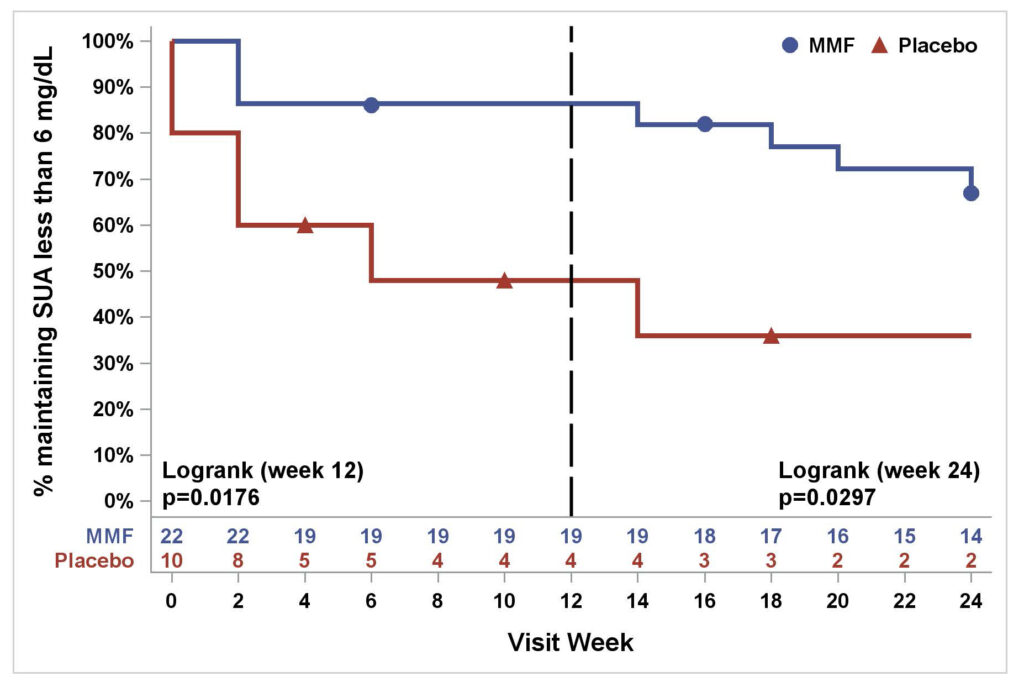
Figure 1. Percentage of subjects maintaining SUA less than 6 mg/dL in MMF/pegloticase vs. PBO/pegloticase arms over 24 weeks (Kaplan‐Meier estimates)
Puja Khanna1, Dinesh Khanna1, Gary Cutter2, Jeffrey Foster2, Joshua Melnick3, Sara Jaafar1, Stephanie Biggers2, AKM Rahman2, Hui-Chen Kuo2, Michelle Feese2 and Kenneth Saag4: 1University of Michigan, Ann Arbor; 2University of Alabama at Birmingham; 3University of Alabama at Birmingham, Vestavia Hills; 4University of Alabama at Birmingham, Division of Clinical Immunology and Rheumatology.
Disclosures: P. Khanna, Selecta, 5, Dyve, 5; D. Khanna, Bayer, 2, BMS, 2, Horizon, 2, Pfizer, 2, NIH, 2, Immune Tolerance Network, 2, Eicos Sciences Inc, 4, Acceleron,, 5, Actelion,, 5, Abbvie,, 5, Amgen,, 5, Bayer,, 5, Boehringer Ingelheim, 5, CSL Behring, 5, Corbus,, 5, Galapagos,, 5, Genentech/Roche, 5, GSK, 5, Horizon, 5, Merck,, 5, Mitsubishi Tanabe Pharma, 5, Sanofi-Aventis, 5, United Therapeutics, 5, Impact PH, 9, Scleroderma Development, 6, CiviBioPharma/Eicos Sciences Inc, 6; G. Cutter, Horizon Pharmaceuticals, 9, Biogen, 5, Click Therapeutics, 5, Genentech, 5, Gilgamesh Pharmaceuticals, 5, GW Pharmaceuticals, 5, Genzyme, 5, Klein-Buendel Incorporated, 5, Medimmune, 5, Medday, 5, Novartis, 5, Osmotica Pharmaceuticals, 5, Perception Neurosciences, 5, Perception Neurosciences, 5, Recursion Pharmaceuticals, 5, Roche, 5, Somahlution, 5, TG Therapeutics, 5; J. Foster, None; J. Melnick, None; S. Jaafar, None; S. Biggers, None; A. Rahman, None; H. Kuo, None; M. Feese, None; K. Saag, Arthrosi, 5, Horizon Therapeutics plc, 2, 5, Atom Bioscience, 5, LG Pharma, 5, Takeda, 5, Mallinkrodt, 5, SOBI, 2, 5, Shanton, 2.
Abstract number 0952, presented at ACR Convergence 2020.
To cite this abstract in AMA style:
Khanna P, Khanna D, Cutter G, Foster J, Melnick J, Jaafar S, Biggers S, Rahman A, Kuo H, Feese M, Saag K. Reducing Immunogenicity of Pegloticase (RECIPE) with Concomitant Use of Mycophenolate Mofetil in Patients with Refractory Gout—a Phase II Double Blind Randomized Controlled Trial [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/reducing-immunogenicity-of-pegloticase-recipe-with-concomitant-use-of-mycophenolate-mofetil-in-patients-with-refractory-gout-a-phase-ii-double-blind-randomized-controlled-trial.