In the emergency department, he was noted to have stable blood pressure of 112/74 and a pulse rate of 130. He received intravenous fluids, pain medications and anti-emetics. He had a CT scan of the abdomen notable for a possible early/partial small bowel obstruction.
While in the emergency department, his labs were notable for a white blood cell count of 14.92, hemoglobin 19.9, hematocrit 58.7 and platelet 353. His creatinine was 1.7, albumin 5.2, bicarbonate 17.2, anion gap 30 and lactate 4.3. (See Table 1)
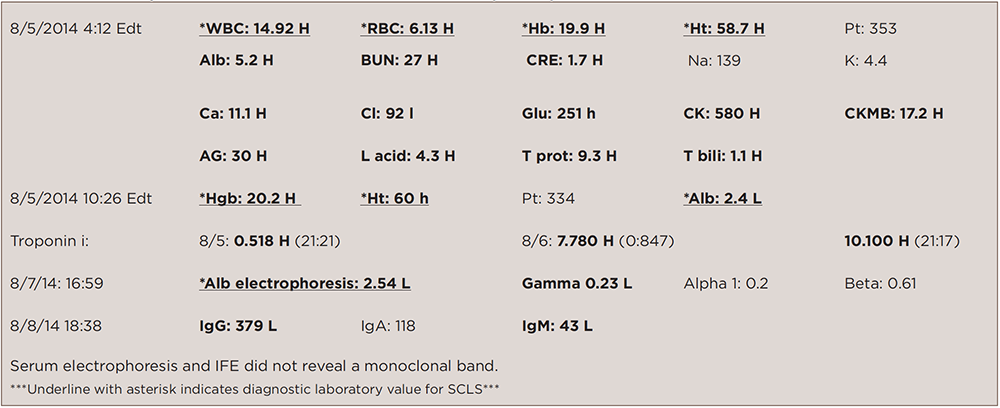
(click for larger image)
TABLE 1: Laboratory Data on Admission & Other Notable Subsequent Inpatient Labs
The patient received 4 liters of intravenous fluids, and within a short amount of time his blood pressure dropped to 69/51. He was immediately transferred to the intensive care unit (ICU). There was concern for sepsis due to ischemic bowel.
In the ICU, he was started on broad-spectrum antibiotics, intubated, given more intravenous fluids with little response, then started on vasopressors. He was taken to the operating room for an explorative laparotomy, which revealed no evidence of perforation.

