(Click for larger image)
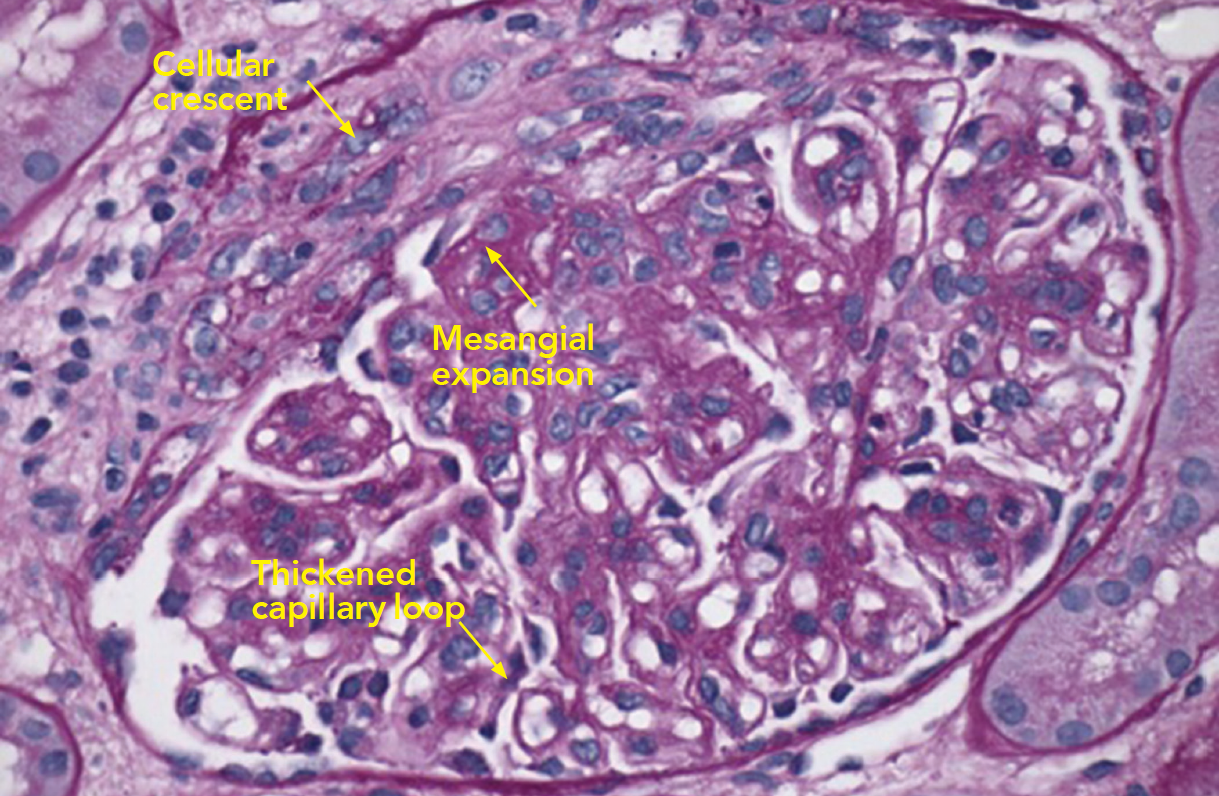
Figure 2: PAS Staining
Example of a glomerulus that contains a focal cellular crescent and expanded mesangium. Thickened capillary loops suggest double contouring of the basement membrane (see Electron Microscopy, Figure 4).
Due to her history of SLE, elevated blood pressure and new-onset nephrotic range proteinuria, the nephrology service performed a kidney biopsy early in her admission to determine if she had developed lupus nephritis. Light microscopy of the kidney biopsy revealed multiple glomeruli containing mesangial expansion and cellular crescents (see Figure 1). Immunofluorescence staining demonstrated faint, granular deposits of IgG and IgM across glomeruli, and C3 along capillary walls (see Figure 2).
In general, lupus nephritis kidney biopsies can exhibit mesangial expansion and cellular crescents, along with strong immunofluorescence staining for IgG, IgM, IgA, C3, C1q, which is known as a “full house.” In this case, the presence of faint granular immunofluorescence and cellular crescents suggested another diagnosis, like ANCA-associated pauci-immune kidney vasculitis.


