(Click for larger image)
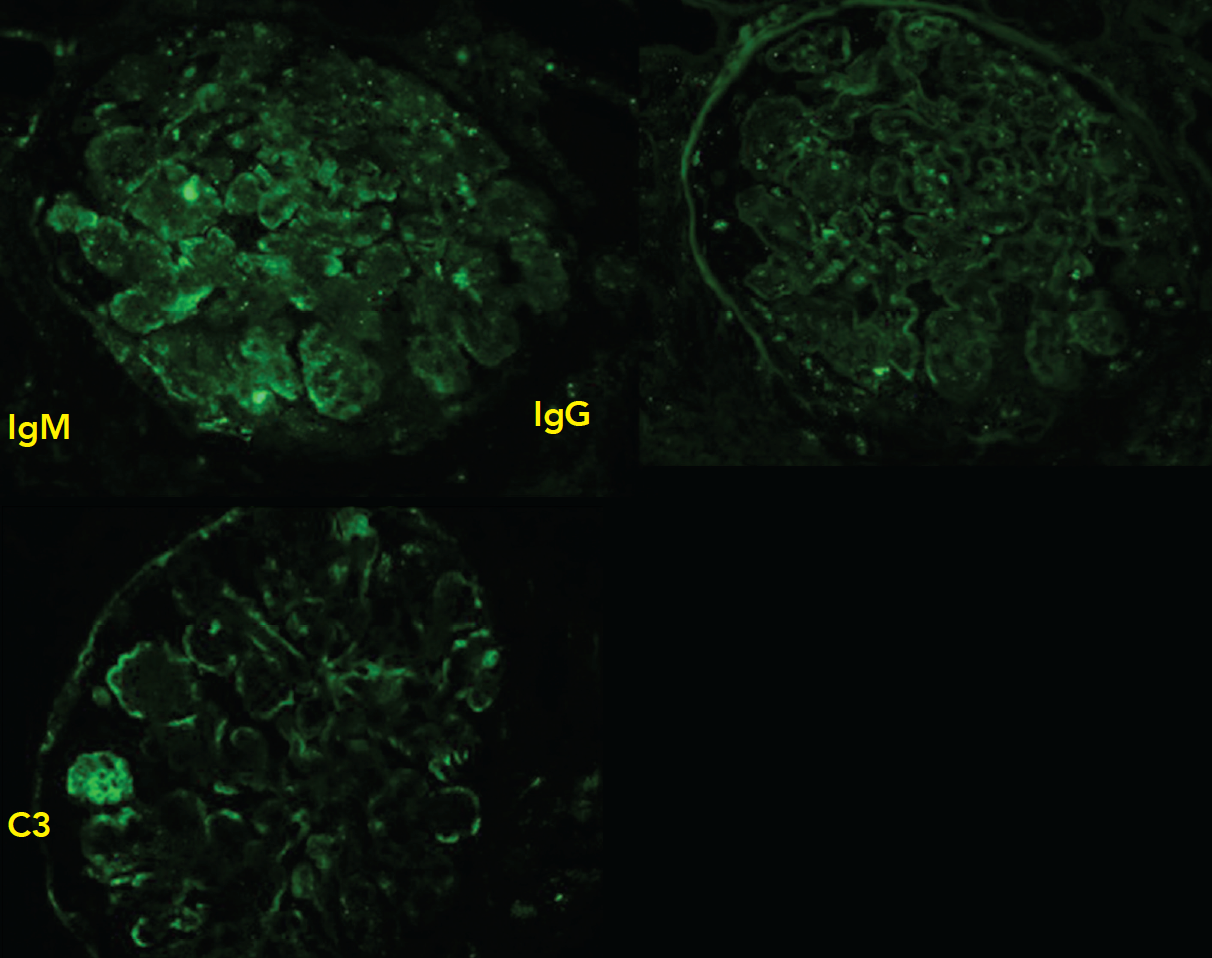
Figure 3: Immunofluorescence
Staining produces faint IgM, IgG diffusely distributed in a granular pattern, while C3 is deposited along the peripheral capillary walls.
Cryoglobulinemia
Cryoglobulinemia is classified into three types that are determined by their immunoglobulin profile. All three exhibit overlapping symptoms, but each is associated with different underlying diseases.
Type I cryoglobulinemia is defined by an isolated monoclonal immunoglobulin. It usually presents with cutaneous ulcers, peripheral neuropathy, arthralgias and kidney involvement (membranoproliferative glomerulonephritis) and is seen with a hematological malignancy or monoclonal gammopathy of undetermined significance.4
Cryoglobulinemia Types II and III generate multiple immunoglobulin classes and are, therefore, known as the “mixed” cryoglobulinemias. Both feature immunoglobulin G, but Type II contains monoclonal rheumatoid factor, and Type III contains polyclonal rheumatoid factor. The mixed cryoglobulinemias present with constitutional symptoms, cutaneous ulcers and kidney involvement. Usually, they are associated with chronic inflammatory states, such as hepatitis C, or autoimmune disorders, such as Sjögren’s, rheumatoid arthritis or SLE.4 In a series of 122 patients with SLE, cryoglobulins were positive in 25% and associated with a higher rate of cutaneous vasculitis.5
Historically, our patient met criteria for SLE on the basis of oral ulcers, pleuritis, positive anti-Smith and ANA. However, several clinical features suggest this presentation was due to cryoglobulinemia, and not SLE activity. Leukocytoclastic vasculitis is commonly seen in cryoglobulinemia, and her complements repeatedly adopted a pattern typical in cryoglobulinemia: low C4 and mildly affected C3. Her double-stranded DNA autoantibody was negative, which is commonly seen in Class III/IV nephritis.4 Interestingly, cryoglobulinemia is not known to correlate with SLE disease activity or nephropathy.5
(Click for larger image)
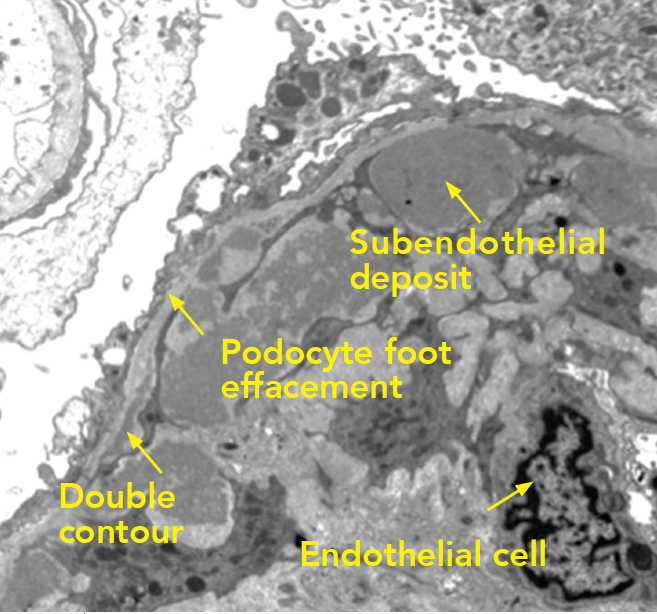
Figure 4: Electron Microscopy
Along the periphery of the capillary loop, the podocyte foot processes are extensively effaced. Segments of the basement membrane adopt a double contour configuration. Inside the basement membrane are subendothelial deposits arranged into small microvesicles or short microtubular structures. The mesangial space is hypercellular and contains increased matrix. Endothelial cells are swollen and lack fenestrations.
2nd Thoughts
This case was educational because we were forced to reconsider the diagnosis by integrating historical clinical information with new serological and biopsy results. As this case demonstrates, SLE, cryoglobulinemia and their associated kidney diseases exhibit overlapping symptoms. Initially, we considered lupus nephritis given her history of SLE and new-onset nephrotic range proteinuria, but our view changed based on the kidney biopsy results and laboratory testing that supported cryoglobulinemia-associated kidney disease. The treatment plan with rituximab did not change, however, because there are data supporting the use of rituximab in cryoglobulinemia.


