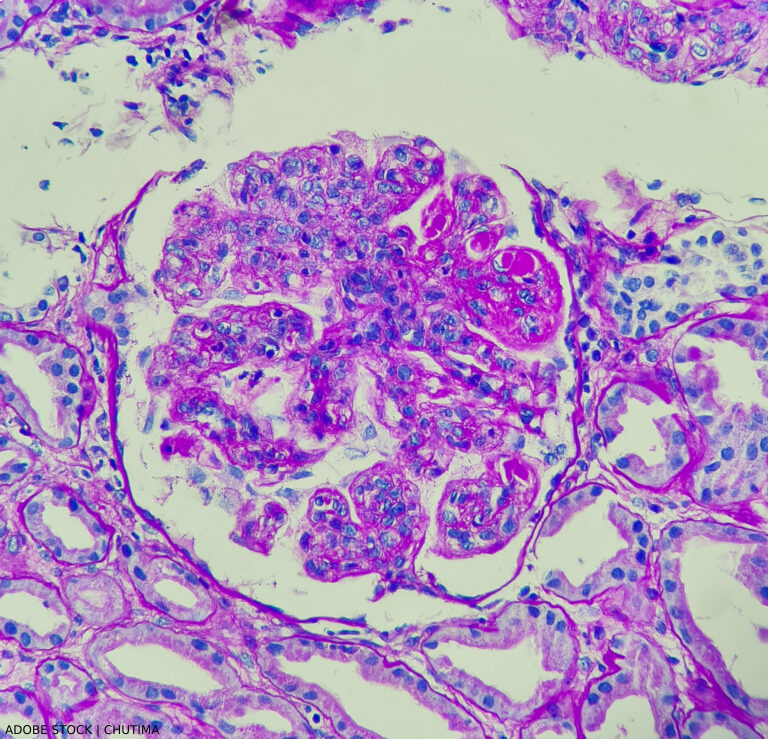
Lupus nephritis, showing wire loop and hyaline thrombi, PAS stain, magnification 400x, photo under microscope.
At a session of ACR Convergence 2024, speakers shared key elements of the new guideline on the screening, treatment and overall management of lupus nephritis in children and adults.1 This guideline attempts to balance the risks of medication side effects with the important goal of preserving kidney function.
This is the ACR’s first lupus guideline since 2012. At that time, recommendations were made for induction therapy with high-dose glucocorticoids plus immunosuppressant medications, such as mycophenolate mofetil (MMF) or cyclophosphamide, with MMF often used as a maintenance therapy.2