The major goal of a DMOAD treatment should be to reduce the progression of joint structural changes, namely cartilage loss. There is a general consensus that a study duration of two years is realistic. The study joint should generally be a weight-bearing one (e.g., knee or hip), unless a specific indication for another joint (e.g., hand) is made. An important issue is whether studying one target joint only is adequate and representative of a drug’s effect. If the effect of treatment is systemic, should more than one joint be studied? This question is of high relevance and needs to be addressed.
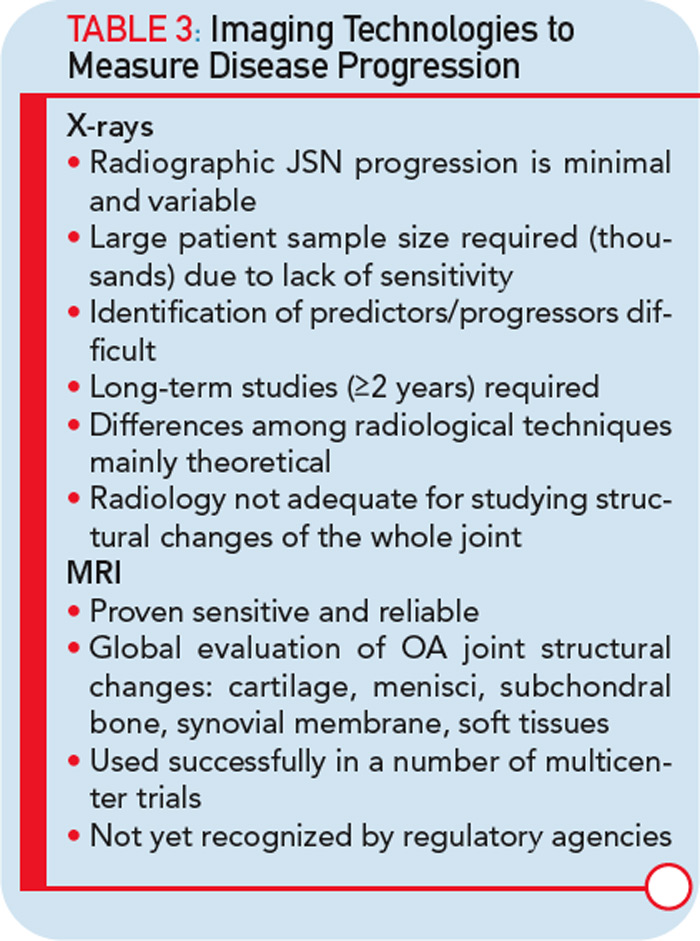
The imaging method used for the assessment of the DMOAD effect has traditionally been X-rays, which are still recommended today. Should this technology still be the gold standard, given the progress made in the field of OA imaging in the last decade? Probably not. This conclusion appears especially true when one realizes the limitations imposed by the use of X-rays (see Table 3).22,23 Advanced technology, such as MRI, can provide more comprehensive and reliable information on the progression of the disease and the effects of DMOAD treatment (see Table 3 and Table 4).20,28,29 MRI is an approved imaging modality and has been used as reference in many fields of research, including trials in cancer and central nervous system disease for a long time. The time has come for the field of OA research to follow suit because this technology can assist in the development of proof-of-concept DMOAD studies and reduce the number of patients to be included in phase II and III trials. Such a change will make DMOAD development programs more affordable and, at the same time, bring new hope to OA patients.
