Posterior Knee Swelling: The Popliteal Cyst
The differential diagnosis of posterior knee swelling includes popliteal cyst, lipoma, aneurysm, thrombophlebitis and muscle herniation due to trauma.1
The most common origin of a popliteal cyst is the bursa beneath the medial gastrocnemius muscle, which may coalesce with another bursa under the semimembranosus tendon to form the gastrocnemius-semimembranosus bursa (GSB).2 The GSB communicates with the healthy native knee joint in 40–54% of the population. 1 When the GSB swells, it is known as a popliteal or Baker’s cyst, named after W. Morant Baker, who described the entity in 1877.3
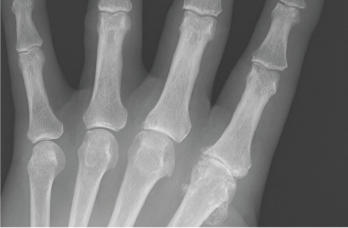
Figure 4: An anteroposterior X-ray of the left hand. Note the metacarpophalangeal (MCP) joint narrowing of digits 2 and 3, osteophytes at the second MCP joint and only mild osteoarthritis at the proximal interphalangeal joints.
Enlargement of the GSB may be primary or secondary.2 Primary GSB enlargement occurs when there is no communication of the cyst to the joint. Inflammatory polyarthritis with direct involvement of the bursal synovium may cause a primary popliteal cyst.2 Secondary GSB enlargement describes synovial fluid flowing from the joint to the cyst via a communicating channel.2 Excess synovial fluid may result from pathology in a native knee, such as a meniscal tear, degenerative change to cartilage, or an inflammatory arthropathy.1,2
Popliteal cysts often present as asymptomatic swelling in the popliteal fossa with or without posterior knee pain. However, continued enlargement of the popliteal cyst may restrict range of motion and compress adjacent structures, such as the popliteal vein, with resultant secondary thrombophlebitis.1,2 Rarely, compression of the tibial nerve may cause neurological dysfunction.4 With continued enlargement, the popliteal cyst may rupture, resulting in severe pain, and can mimic thrombophlebitis.1,2



