During the session, entitled “Kawasaki Disease: Putting Out the Fire,” a panel of experts provided updated information on the diagnosis and treatment of KD with an emphasis on the need for early detection to minimize complications, including the potential for the formation of coronary artery aneurysms.
Kawasaki Disease: What It Is and What It Is Not
Knowing how to recognize KD and make the differential diagnosis from other diseases is not easy, and requires familiarity with an evolving understanding of what the disease is, according to Robert Sundel, MD, program director in rheumatology at Boston Children’s Hospital, and associate professor of pediatrics at Harvard Medical School in Boston. He emphasized the limitations of the classic or traditional criteria once used to diagnose KD, and discussed more recently developed modified criteria that expanded the differential diagnosis of KD (see Table 1).
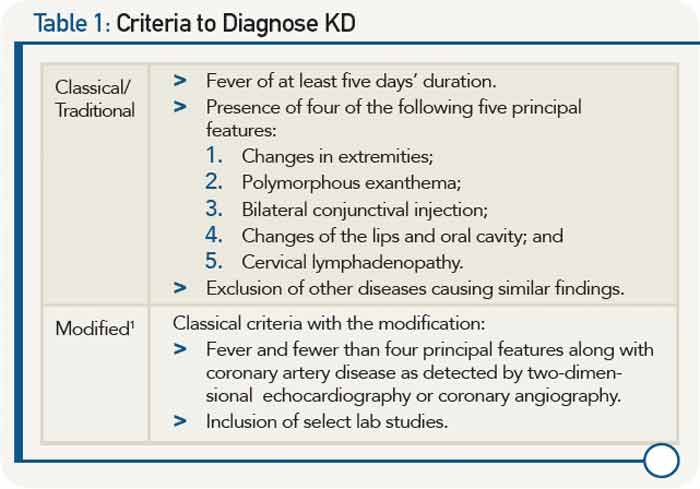
Among key features that led to formulation of the modified criteria was the recognition that many patients with KD have concurrent infections, complicating determination of which other conditions to consider in the differential diagnosis. Further, evolving recognition of cardiac involvement in patients who do not meet classical criteria for KD necessitated alternative approaches to optimize outcomes. Occult cardiac involvement in patients with KD includes myocarditis and, importantly, coronary artery aneurysms, he said, emphasizing that the presence of cardiac involvement is a major prognostic determinant with a mortality rate of 1.5% in untreated patients that falls to less than 0.1% in treated patients.