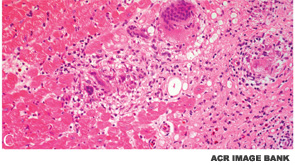
BOSTON—Diagnosis of both cardiac sarcoidosis and neurosarcoidosis requires a process of exclusion and a high degree of clinical suspicion, according to a presentation at the ACR/ARHP Annual Meeting in Boston in November 2014, Sarcoidosis in 2014. Akin to problems associated with the general diagnosis of sarcoidosis, there is no one reliable diagnostic test for either condition, the clinical manifestations can be nonspecific, and there are no evidence-based guidelines for treatment.
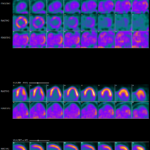
Daniel Culver, DO, a pulmonologist at the Cleveland Clinic, said diagnosis of cardiac sarcoidosis can be difficult and should include a finding of sarcoidosis in an organ outside the heart and presence of a heart lesion that cannot be explained by other causes. A patient’s symptoms, however, are still the most important for diagnosis.