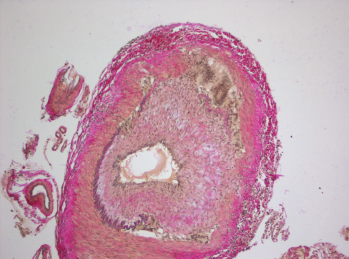
Histopathology of giant cell arteritis in a temporal artery.
wikimedia.org
A recent study, conducted by the Vasculitis Clinical Research Consortium and funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), examined whether the addition of abatacept, a drug that affects T cell activation, to standard prednisone treatment could reduce the risk of relapse in patients with giant cell arteritis (GCA).1 Although abatacept has been approved by the FDA to treat rheumatoid and juvenile idiopathic arthritis, there had been no prior experience with its use as a treatment option for GCA.
Carol Langford, MD, MHS, of the Center for Vasculitis Care and Research at Cleveland Clinic, and the study’s lead investigator, discussed the reasons why the study of abatacept was pursued in GCA: “Abatacept inhibits T cell activation, which is thought to play a critical role in the pathogenesis of GCA,” Dr. Langford says. “Because of this mechanism, its favorable safety profile in rheumatoid arthritis and the unmet need for additional treatment options in GCA, abatacept was an interesting drug to investigate.”

