
Frequently, I hear about colleagues who are looking for a partner to join their busy practice, a scientist to join their units or even for a chief to lead their division. Although I know the statistics of supply and demand in rheumatology, I am amazed at how the demand seems to outstrip the supply of rheumatologists and rheumatology professionals.
The ACR continues to work toward increasing, strengthening and diversifying our subspecialty through many initiatives. One component of this effort is data collection about the workforce and the practice of rheumatology to keep the ACR and its members informed. Information is power.
I would like to focus this month’s column on the ACR Benchmark Tool—specifically, the data collected using the 2012 Benchmark Tool and the changes to the Benchmark Tool that will begin in 2014.
Angus Worthing, MD, Arthritis and Rheumatism Associates, Washington, D.C., participated in the first ACR benchmark survey & says he also plans to participate when the new tool opens. ‘I encourage all my colleagues to make time to complete the survey when it opens in September so the ACR can gather & provide the most up-to-date data nationwide on practicing rheumatologists,’ he says.
The ACR’s fundamental purpose for this project is to Advance Rheumatology! by ensuring an adequate rheumatology practice environment and workforce in an era of increased prevalence of chronic musculoskeletal diseases. The Benchmark Tool has the potential to be the ACR’s primary source of member-reported data and could aid in our overall goals of developing tools to address evolving payment reforms, improving practice costs and efficiency, enhancing quality of care, and strengthening research and training in rheumatology. To pursue these goals with any vigor, we need a complete database, and that requires your participation and a bit of your time. Its utility depends on all of us reporting accurate data.
Highlights from the 2012 Benchmark Tool
The most recent ACR Benchmark Tool was released in February 2012, and by the time it closed in February 2014, only 682 physicians had answered all or even just some of the questions. I will discuss some trends that were suggested from an analysis of these responses. A full report of the data collected during this period is available to all ACR members by logging in and accessing the My Profile section.
The primary employment setting for survey respondents was:
- 35.7%—Academic Medical Center
- 19.3%—Multi-Specialty Group Practice
- 16.4%—Single Specialty Group Practice
- 15.3%—Solo Practice
- 5.5%—Hospital-Based Practice
- 2.6%—Government Clinical Setting (VA)
- 1.5%—Other Clinical Setting
- 1.5%—Biomedical Industry
- 1.4%—Retired
- 0.5%—Government Non-Clinical Setting
- 0.5%—Other Non-Clinical Setting
Because the majority of our members are in clinical practices, these data do not represent a typical cohort of our ACR constituency. You can help us accumulate more representative information, by completing the 2014 version of the Benchmark Tool when it’s launched in September.
The majority of respondents (62.6%) reported a yearly compensation in the range of $150,001–350,000. Twenty-seven percent of respondents reported a yearly compensation of less than $50,000–150,000, and 10.2% reported $350,001–500,000 plus. When more ACR members provide their income data, we will be able to use it as a resource in measuring our productivity relative to our peers.
Demand
More than half of the respondents reported working more than 50 hours per week, some as much as an incredible 81 hours or more per week! Although this may be true, it certainly doesn’t reflect the lifestyle of the “happiest subspecialty,” as rheumatology is reported to be, no matter how much we enjoy our work. During a fully scheduled workweek, more than 70% reported seeing 20 or fewer new patients. Twenty-eight percent indicated more than 20 new patient visits per week, and 1.3% of that group reported seeing an energetic 121–140 new patients in one week. Nearly 54% of the survey respondents reported 41–80 return patient visits during a typical workweek.
Do the new patient visits and work hours reported from the population who completed the survey tool mirror yours?
Clinical Practice
Ninety-four percent of rheumatologists reported their practice is dedicated to adult rheumatology. The report shows that a majority of rheumatology practices don’t provide significant primary care services.
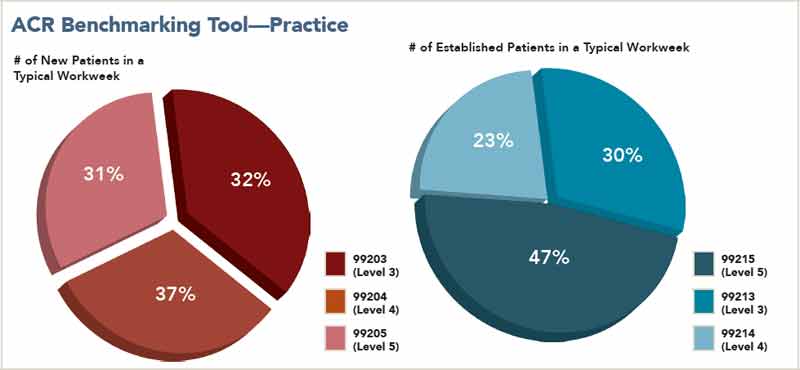
As in the 2009 report (see pie charts), rheumatologists in private practice said nearly three-fourths of their compensation comes from direct patient care.
Of the practicing rheumatologists who participated, 62% reported they code a Level 3 (99203) new patient visit in a typical workweek, 71% reported billing Level 4 (99204) visits, and 61% reported billing a Level 5 (99205) new patient visit in a typical week. Additionally, 38% reported they bill Level 3 (99213) established patient visits in a typical week, 31% bill Level 4 (99214) visits, and 60% bill Level 5 (99215) visits in a typical workweek. This may reflect the complex array of patients managed by rheumatologists.
Academic
Of the academic rheumatologists who completed the survey (see pie charts at right), 62% reported clinical care as their predominant source of payment, and 26% indicated investigator-initiated research was the primary source of the majority of their income. Of that group, 47% selected clinical care as their primary professional activity, and 41% reported their primary activity as either clinical or basic research.
The discrepancy between sources of income and amount of time spent indicates that funding for research is insufficient to support the time spent in the activity. Only 9% of academic rheumatologists who responded to the survey have received NIH support during their career. The NIH award mechanism that was the most common among respondents is the R01 award, with 21.8% indicating they have received one. This was sobering data for me when I first saw it, but it reflects the crisis in academic rheumatology research.

The New & Improved 2014 Benchmark Tool
Beginning in 2014, the new version of the ACR Benchmark Tool will transition from a rolling survey format to a yearly collection of data. The tool will be open for responses for a three-month period each year. The smaller window to complete the survey will strengthen the integrity and timeliness of data collected. It will also demand timely responses from practices.
The next version of the tool is expected to be available Sept. 1 through Dec. 1, 2014. The ACR will alert members once the tool is open for responses. It will be available online to complete when you find it convenient. You may also complete the survey on site in November at the Annual Meeting at kiosks stationed there. If you choose this option, you will need the data from your practice available to you at the meeting.
Angus Worthing, MD, Arthritis and Rheumatism Associates, Washington, D.C., participated in the first ACR benchmark survey and says he also plans to participate when the new tool opens. “I encourage all my colleagues to make time to complete the survey when it opens in September so the ACR can gather & provide the most up-to-date data nationwide on practicing rheumatologists,” he says.
The link to take the Benchmark Tool and to access results after completing the tool will be available in each ACR member’s My Profile section on the ACR website. Once you have filled out the Benchmark Tool, you will have the ability to see how your enterprise compares in each aspect with others regionally and nationally. The data from other practices will, of course, be de-identified. If you completed the 2012 Benchmark Tool, I’m sure you found that having the ability to view your performance and your practice’s activities compared with others in your region and across the country can be very useful.
The ACR Benchmark Tool is a superb resource to help the ACR collect & analyze data on the rheumatology workforce & identify local & membership-wide trends & performance issues that can be addressed by the ACR & its committees. I hope each ACR member will complete the 2014 Benchmark Tool when it is released in September, so the ACR can better serve the needs of the rheumatology workforce.’
The 2012–2014 Benchmark Tool offered a good opportunity to further beta test the concept of the tool and its elements. But because so few members completed it, it does not yet have the power it should have to help us gauge our performance relative to our peers. ACR’s challenge is to discover what will motivate us to make the time to contribute to this potentially powerful information database.
The survey has the promise to give you the information you need to ensure the survival of your practice and to allow you to continue to thrive. We are at the threshold of mammoth reversioning of medical practices and investigation. Perhaps we are in rheumatology version 2.0 or maybe 10.0. The Benchmark Tool can help you leverage yourself or your organization in the next version.
The ACR will carefully analyze these data to publish a report summarizing the information each year and this de-identified report will be made available to the ACR membership. Our hope is that information gathered by the tool will lead to projects aimed at addressing workforce development, evolving payment reforms, increasing practice efficiency and improving quality of care.
“The ACR Benchmark Tool is a superb resource to help the ACR collect and analyze data on the rheumatology workforce and identify local and membership-wide trends and performance issues that can be addressed by the ACR and its committees,” says Marcy B. Bolster, MD, Massachusetts General Hospital, Boston, and chair of the ACR Committee on Rheumatology Training and Workforce Issues. “I hope each ACR member will complete the 2014 Benchmark Tool when it is released in September, so the ACR can better serve the needs of the rheumatology workforce.”
I strongly encourage everyone to complete the 2014 ACR Benchmark Tool when it becomes available in September. It’s imperative that we increase participation in order to track practice trends and workforce supply over time and identify issues being faced by rheumatologists nationwide. The more members who participate, the more representative and useful the deductions the ACR can make about the health of our subspecialty and the conclusions about your own situation relative to your peers. Your participation will Advance Rheumatology!
Dr. Joseph Flood is a rheumatologist at the Columbus Arthritis Center and adjunct associate professor at The Ohio State University College of Medicine and Public Health, both in Columbus. Contact him at [email protected].