During the ophthalmology visit, the patient should be dilated for at least 30 minutes with cyclopentolate 1% and phenylephrine 2.5% drops for a detailed examination of the retina and measurement of refractive error. Measurement of refractive error when the pupils are dilated is essential in all children, especially those with reduced visual acuity, to determine whether vision changes are related to refractive error or amblyopia.
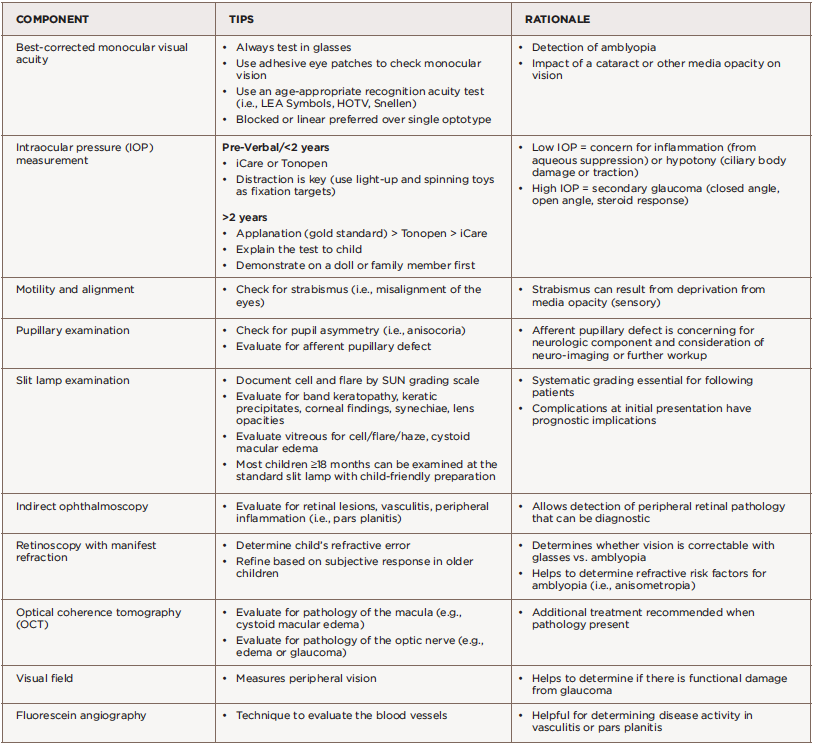
(click for larger image) Table 3: Eye Examination Components
Amblyopia is decreased vision in one or both eyes due to abnormal visual stimulation of the brain in infancy or early childhood. Uveitis can cause amblyopia via changes in refractive error from lenticular changes, glaucoma or deprivation secondary to media opacities such as band keratopathy, cataract, vitreous opacities and cystoid macular edema. Ancillary testing by visual field test (to measure peripheral vision), optical coherence tomography (to measure the thickness of the optic nerve and macula), and fundus photography may be performed based on clinical examination findings. This testing can help monitor complications of uveitis, such as glaucoma or cystoid macular edema.


