After rheumatology evaluation, treatment with high-dose oral steroids (prednisone 1 mg/kg daily) was initiated and patient was referred back to ENT for sinus biopsy. The pathology report was consistent with granulomatous vasculitis and necrosis involving sinonasal mucosa, revealing extensively inflamed and ulcerated sinonasal tissue with dense lymphoplasmacytic infiltrate and granulation tissue formation. Occasional profiles of medium-size arterioles show infiltration by lymphocytes and occasional giant cells (see Figures 1 and 2).
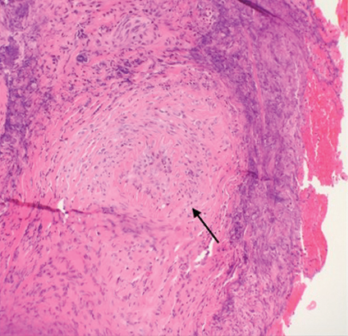
Figure 1. A nasal biopsy shows intimal infiltration of the small blood vessels (black arrow).
To evaluate disease extension, a CT of the chest was obtained. No hilar or mediastinal adenopathy, lung nodules or pleurisy were noted. An audiogram was also performed and was negative for hearing loss.

