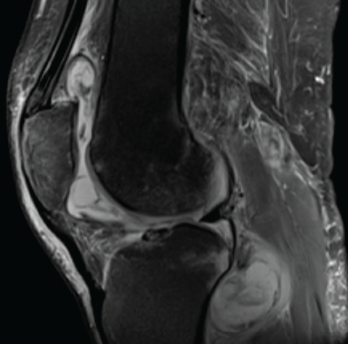
Figure 1. Magnetic resonance imaging of the patient’s left knee shows joint effusion, synovial thickening, and periarticular muscle and soft tissue edema.
Tumor necrosis factor-α inhibitors (TNFi’s) have emerged as an integral part of therapeutic strategies for several rheumatic diseases. TNF-α is a pro-inflammatory cytokine implicated in the pathogenesis of rheumatoid arthritis (RA), seronegative spondyloarthropathies and inflammatory bowel disease (IBD). It also plays a central role in the immune response to mycobacterial infection.
Many biologic agents, particularly TNFi’s, are associated with an increased risk of tuberculosis; however, the risk of non-tuberculous mycobacterial infections among patients treated with a TNFi has not been studied extensively.