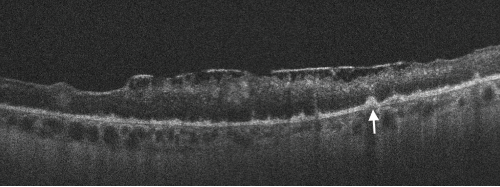
Figure 2. Spectral domain optical coherence tomography (SD-OCT) of the left eye with hyper-reflective retinal pigment epithelial (RPE) nodularity (white arrow) and overlying loss of normal photo receptor architecture.
Discussion
Ocular syphilis is rare and tends to occur at any stage of the disease. However, it is commonly associated with neurosyphilis. Its incidence has been increasing in the developed countries for the past few years. This may be related in part to decreased condom use in high-risk populations following the advent of highly active anti-retroviral therapy (HAART).5
Because its clinical manifestations vary, ocular syphilis is a big masquerader and may be challenging to diagnose. Ocular symptoms are commonly non-specific and may lead to a delay in diagnosis and treatment. New-onset, monocular, blurry vision is usually an early manifestation; however, other non-specific systemic symptoms can mask the diagnosis.


