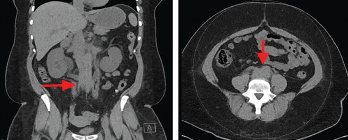
Figure 3. Computed tomography (CT) scan of the abdomen and pelvis (left panel: coronal view; right panel: axial view), without intravenous contrast administration, demonstrating increased retroperitoneal density around the aortic bifurcation (arrows).
The patient underwent retrograde pyelography, which confirmed bilateral hydronephrosis. A double-J stent was placed on the left kidney; because of the fishhook configuration of the right ureter, a nephroureteral stent was placed in the right kidney with subsequent conversion into a double-J stent.
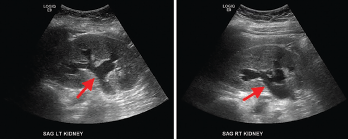
Figure 4. Renal ultrasound, sagittal view, showing bilateral grade 2 hydronephrosis (arrows) with normal renal cortical thickness and without focal lesions or nephrolithiasis.
A follow-up ultrasound demonstrated resolution of the obstruction (see Figure 5). Additional laboratory tests (see Table 1), including anti-nuclear antibody (ANA), anti-neutrophil cytoplasmic antibody (ANCA), complement, immunoglobulin levels, serum protein electrophoresis (SPEP) and immunofixation (IFE), were all unremarkable.
A clinical diagnosis of idiopathic retroperitoneal fibrosis leading to obstructive uropathy was made, and induction therapy with 1 mg/kg/day of prednisone was initiated. She responded well, and, at the time of discharge, her serum creatinine was 1.3 mg/dL; her improvement in serum creatinine was presumed to be due to stent placement and glucocorticoid therapy.
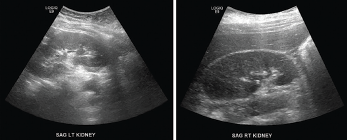
Figure 5. Renal ultrasound, sagittal view, performed a week after stenting showed complete resolution of hydronephrosis.
Discussion
RPF is a rare inflammatory disease often associated with non-specific clinical features; its etiopathogenesis is poorly understood.1 The overall incidence of RPF is unknown. Previous studies have estimated the incidence of idiopathic RPF at approximately 0.1–1.3 cases/100,000 people/year and the prevalence at approximately 1.4 cases/100,000 people.1 RPF is often diagnosed in patients between the ages of 40 and 60 years. Some studies have shown a 2:1 to 3:1 male predominance.1 It is possible that a higher number of male patients seek medical attention due to the genitourinary symptoms and, therefore, men may be over-represented in these studies.3

