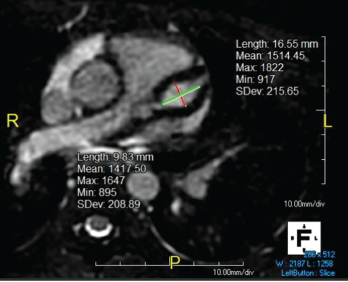
Figure 1. Giant LAD fusiform aneurysm measuring 9.8 mm in diameter (z-score = 19) and extending approximately 17 mm.
In September 2019, a previously healthy, 9-year-old white girl presented to the emergency department following two months of sinusitis and unexplained fever responsive to ibuprofen. She presented with anorexia; a 9 lb. weight loss; intermittent, nonbilious, nonbloody emesis; and occasional epistaxis with digital manipulation of the nose.
Six weeks prior to admission, she had presented to the emergency department with fever and rhinorrhea unresolved by amoxicillin. An evaluation revealed an erythrocyte sedimentation rate (ESR) of 58 mm/hr (reference range [RR] 0–20 mm/hr), a C-reactive protein (CRP) level of 22 mg/L (RR: 0–9 mg/L), a white blood cell (WBC) count of 17.6 cells/μL (RR: 5.4–9.7 cells/μL) and a hematocrit level of 41% (RR: 35–43%). A chest radiograph was unrevealing, and the urinalysis was normal, demonstrating a baseline creatinine (Cr) level of 0.4 mg/dL (RR: 0.31–0.61 mg/dl). She tested positive for enterovirus and was sent home with conservative management.