Diagnosis & Treatment
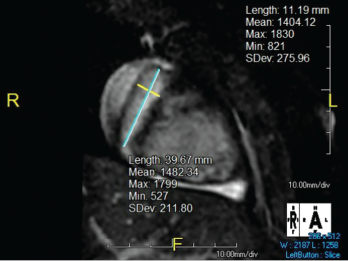
Figure 2. The right coronary artery sustained a giant fusiform aneurysm 11 mm in diameter (z-score = 20) and 40 mm in length.
The patient was diagnosed with granulomatosis with polyangiitis (GPA) and started on 1,000 mg of pulse dose intravenous methylprednisolone daily for three days and 81 mg daily of aspirin.
Sinus computerized tomography (CT) showed mucosal thickening and “bubbly” fluid in the sphenoid sinuses. A chest CT showed pleural effusions and potential upper lung nodules measuring 5 mm. A percutaneous biopsy of the left kidney revealed severe necrotizing crescentic pauci-immune glomerulonephritis.