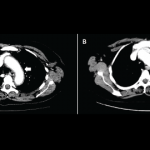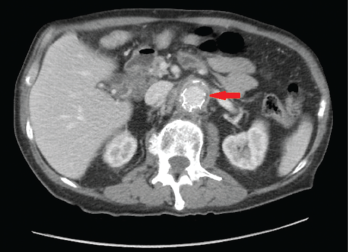
Figures 1A & 1B (below): A CT scan with abdominal and pelvic axial (a) and sagittal (b) views showing inflammatory changes (red arrow) adjacent to the aorta.
A 76-year-old Caucasian male with a history of abdominal aortic aneurysm repair five years earlier presented with three months duration of worsening periumbilical abdominal pain associated with nausea, non-bloody emesis, decreased appetite, fatigue and a 40 lb. weight loss. He denied having fever, chills, night sweats, temporal headaches, vision loss, chest pain, shortness of breath and jaw, upper and lower extremity pain.
On physical exam, the patient had no temporal artery tenderness. His peripheral pulses were normal and symmetric. The abdominal exam was significant for tenderness in the left periumbilical region with no guarding or rebound tenderness.
Laboratory analysis revealed a white blood cell count of 10.7 k/mm3, hemoglobin level of 11.1 g/dL and platelets at 294 k/mm3. The sedimentation rate of 140 mm/hr was elevated (normal: 0–22 mm/hr), as was the C-reactive protein level at 23.2 mg/L (normal: 2.0–8.0 mg/L). The creatinine level was normal at 0.93 mg/dL (normal: 0.6–1.50 mg/dL). The albumin level was low at 2.2 g/dL (normal: 3.4–5 g/dL).
A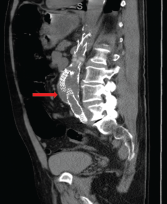 computed tomography (CT) scan of the abdomen and pelvis with contrast showed wall thickening and adjacent fat stranding involving the abdominal aorta and proximal bilateral common iliac arteries at the level of endovascular stent for the abdominal aortic aneurysm (see Figures 1a and 1b, right). These findings were suspicious for aortitis.
computed tomography (CT) scan of the abdomen and pelvis with contrast showed wall thickening and adjacent fat stranding involving the abdominal aorta and proximal bilateral common iliac arteries at the level of endovascular stent for the abdominal aortic aneurysm (see Figures 1a and 1b, right). These findings were suspicious for aortitis.