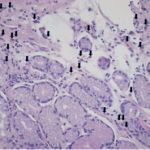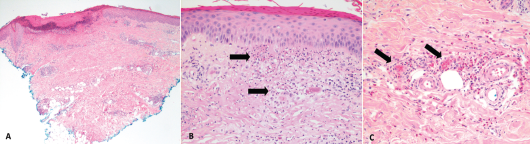
Figure 2. These hematoxylin and eosin stain images show the patient’s histology of RCEV demonstrating vasculitis, including image A, a biopsy from her right leg showing ulceration and superficial and deep perivascular inflammation with vascular damage (magnification 40X); B, a biopsy from her left leg showing cutaneous small vessel vasculitis (the arrows indicate examples of damaged blood vessels) with fibrinoid necrosis of vessel walls and surrounding nuclear debris/leukocytoclasis (magnification 200X); and C, a biopsy from her right leg showing small vessel vasculitis (arrows), uninvolved adjacent small arterioles and abundant perivascular and interstitial eosinophils (magnification 200X).
Discussion
RCEV was initially described by Chen et al. in 1994 and is characterized clinically by its benign course and classically pruritic skin eruptions. Various skin morphologies have been noted with RCEV, including urticaria, papules, patches, nodules, angioedema and vesicles.1-9 Only one previous group has described RCEV with ulcerating lesions, as we saw in this case.8 The lack of peripheral eosinophilia noted in our case was also unique, and this feature was noted in only three of the 17 cases.4,6,9
Histology can reveal necrotizing vasculitis with predominant eosinophilic infiltration, and others have commented on the presence of neutrophils and lymphocytes.5,8,9 Granulomas and leukocytoclastic features are typically absent in RCEV, although our case did feature some evidence of leukocytoclasis on histology.1-9 A number of specific findings enabled us to rule out similar conditions, such as eosinophilic granulomatous polyangiitis (EGPA), urticarial vasculitis, Wells syndrome and hypereosinophilic syndrome (HES).