Hospital Course
On admission—two months after her first emergency department visit—her physical examination showed proptosis of the right eye with slight edema, compared with the left eye. This was a new finding. Despite the proptosis and mild edema, extraocular movements were intact. She did have lymphadenopathy that was worse along the right side of her neck. Otherwise, the examination was unremarkable. During questioning, she said she began to have blurry vision while in the emergency department that day.
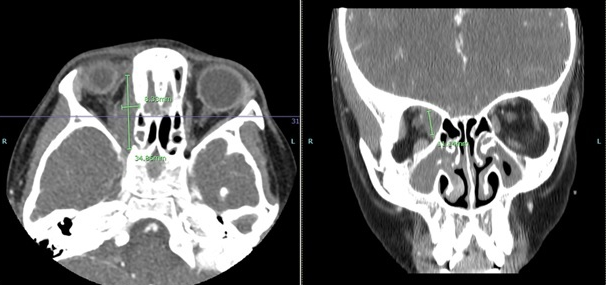
FIGURE 1. Click to enlarge.
Magnetic resonance imaging (MRI) showed a right medial, orbital mass encasing the right trochlear and medial rectus muscles (see Figure 1). The mass was non-uniform, with variable signal intensity. Again, imaging favored a non-infectious inflammatory process over infection. Pansinusitis with osseous destruction of the medial maxillary sinus walls was visualized on the right. The laboratory testing was expanded to include IgG subclasses to evaluate for IgG4 disease; all IgG subclasses were elevated (see Table 1).


