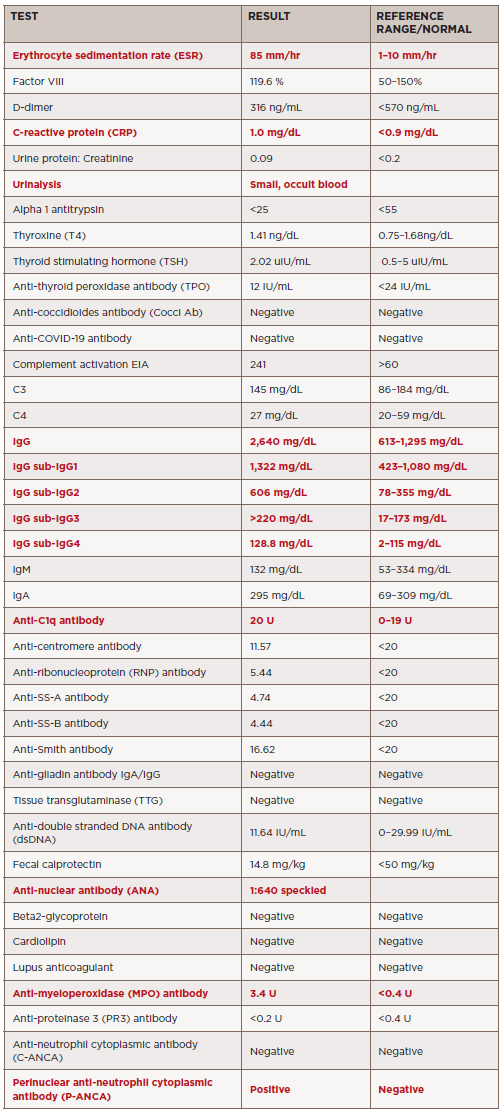
TABLE 1. Summary of laboratory results. Abnormal results indicated in red.
After diagnosis, the patient received pulse therapy with glucocorticoids (30 mg/kg/dose = 800 mg) for three days and then transitioned to 20 mg of oral prednisone twice a day, followed by a prednisone wean. She was given rituximab induction therapy (750 mg x two doses, two weeks apart) followed by maintenance therapy (thus far receiving one dose). Currently, she has been weaned off prednisone and is doing well overall, with minimal symptoms.
A follow-up MRI eight months later showed markedly decreased orbital mass, with only a small residual area of enhancement between the right medial rectus and superior oblique muscle. There was also slightly decreased pansinusitis, with osseous destruction of the medial maxillary sinus walls and dehiscence of the right lamina papyracea. Further, the anterior cranial fossa pachymeningeal thickening and enhancement was nearly resolved.


