Low Complexity
The medical decision making (MDM) component is part of the evaluation and management (E/M) level of coding that refers to the complexity of establishing a diagnosis and/or selecting a management option, which is measured by:
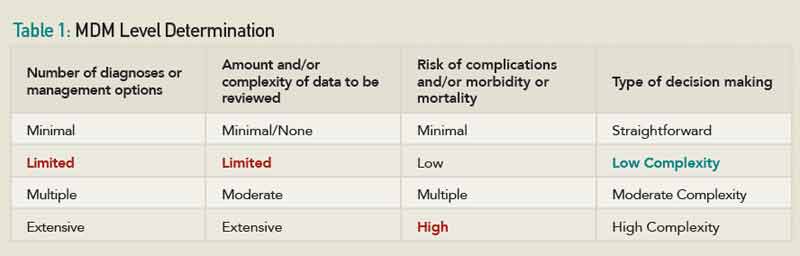
- The number of possible diagnoses and/or the number of management options that must be considered. There are two problems addressed in the patient’s assessment, and each is listed as stable. Two established, stable problems equal two points. An established stable problem is weighted as one point, and an established worsening problem is weighted as two points. The level of the number of diagnosis or treatment options is measured by what is wrong with the patient on the date of service. Therefore, this section of the MDM would be listed as limited.
Note: When payers review claims data on MDM, it is weighted on a point system that is used to reach a final level of an E/M service. - The amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed. The amount of data reviewed and/or ordered for this visit equals two points—one point for the labs reviewed and one point for the dual-energy X-ray absorptiometry diagnostic test ordered. This equals two points, making this element of the MDM limited.
- The risk of significant complications, morbidity, and/or mortality, as well as comorbidities, associated with the patient’s presenting problem(s), the diagnostic procedure(s), and/or the possible management options. Because the drug therapy requires intensive monitoring for toxicity, the level of risk is high.
Only two out of three components are needed to determine the MDM level. The medical decision making is of low complexity. Table 1 summarizes the process of determining the MDM level.
When it comes to reimbursement, MDM usually drives the level of the visit. The MDM supports the medical necessity for a patient’s visit on the date of service. Physicians should be aware that while, technically, you only need two out of three of the history, examination, and MDM to determine the level, MDM should be one of the two. For example, the achievement of a comprehensive history level and a comprehensive examination level, but with low MDM, would not support the medical necessity of a level-four or -five visit.
For questions or additional information on coding and billing, contact Melesia Tillman, CPC, CPC-1, CRHC, CHA, at [email protected] or (404) 633-3777, ext 820.

