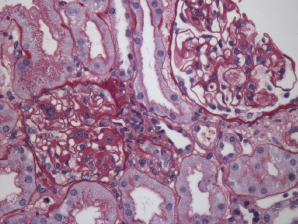
Figure 2. Renal biopsy showing class III lupus nephritis with rare foci of subendothelial deposits (wire loop lesions).
Due to his persistent pancytopenia, the consulting hematologist performed a bone marrow biopsy that did not demonstrate evidence of a malignancy. Within a week of his admission, his creatinine increased to 2.46 (mg/dL) from 0.98 (mg/dL) with a urinalysis that demonstrated mild hemoglobin and albumin. A renal biopsy was performed; it demonstrated evidence of lupus nephritis class III (see Figure 2). Approximately three weeks later, he was also found to have anti-double-stranded DNA antibodies.
The patient was started on prednisone 60 mg daily, hydroxychloroquine 400 mg daily and mycophenolate mofetil 2 g daily.