Take Home Points
- Antisynthetase syndrome may present without muscle involvement.
- Careful attention should be paid to the skin examination.
- Antisynthetase antibody testing, particularly anti-Jo-1, should be performed in all patients with ILD without an obvious etiology because pulmonary involvement may be the sole presenting manifestation.
- Coexistent SSA positivity is a marker of more severe lung disease.
The Case
A 24-year-old white male was seen in July 2012 because of multiple complaints. He had been doing well until three weeks earlier, when he developed pain and diminished hearing in his left ear, which was accompanied by cough and a postnasal drip. He had had two tympanostomies due to left ear problems in the past, and attributed the current symptoms to the same problem.
One week later, he developed pain and swelling in multiple joints. The joint pain was of sudden onset and involved his shoulders, wrists, fingers, and feet. He could not make a fist due to the pain and swelling.
One week later, he complained of shortness of breath and described two episodes of hemoptysis—a tablespoon full of bright red blood each time—that brought him to a community hospital. He felt warm but denied any chills, night sweats, or weight loss. He recalled removing a dead flat tick from his back a few days earlier. He was treated with doxycycline and a five-day course of prednisone for a presumed tick-borne illness. The prednisone improved his joint pain and swelling. He was an otherwise healthy male. He occasionally took antihistamine pills for treatment of nasal allergy symptoms.
His father had severe rheumatoid arthritis (RA) and his mother was recently diagnosed with sarcoidosis. He was married without children and denied smoking, alcohol, or illicit drug use. He denied any extramarital sexual activity. He worked as a taxidermist and was exposed to oxalic acid, tannic acid, and some other oils. He had no pets. Travel history was unremarkable.
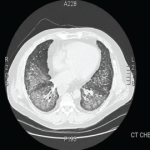
After the five-day course of prednisone 20 mg, he continued to cough but denied hemoptysis. Joint swelling and pain recurred. At the community hospital, a chest radiograph showed interstitial and alveolar infiltrates and bilateral pleural effusions. He underwent a bronchoscopy and a bronchoalveolar lavage (BAL), which was negative for any infection. Results for acid-fast bacilli and serologies for common tick-borne diseases were negative. Intravenous vancomycin and ceftriaxone were administered for possible pneumonia. He continued to have joint pains and was referred to our facility on his third hospital day.