Implementation
A change in habits and attitudes is critical to implementing these recommendations,

Dr. Dasgupta
according to Dr. Dasgupta. “These [recommendations] are the first steps to introduce the scientific method in the management of this condition,” he says, emphasizing that clinicians need to accept flexible dosing for PMR.
Dr. Dasgupta says the current recommendations are part of a continuum of activity over the past several years to address the need for better uniformity and standards in the management of PMR. Efforts have included a commentary published in Arthritis & Rheumatism in 2006 highlighting the need for better guidance and standards, and subsequent guidelines for the management of giant cell arteritis issued in 2010 by the British Society for Rheumatology and British Health Professionals in Rheumatology, as well as the EULAR/ACR classification criteria for PMR issued in 2012.3-6
(click for larger image)
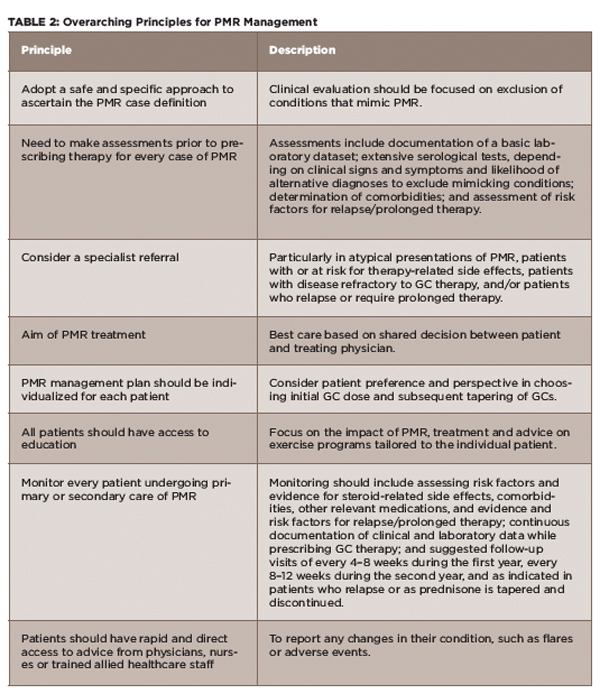
TABLE 2: Overarching Principles for PMR Management
Source: Adapted from Dejaco et al 20151
With the new recommendations, Dr. Dasgupta stresses the importance of carefully assessing each patient with suspected PMR and tailoring treatment according to the specific individual. This includes individualizing steroid dose, a gradual tapering of steroids, early introduction of DMARDs, such as methotrexate, to avoid NSAIDs and the occasional need for intramuscular methyprednisolone in patients who require lower cumulative doses. He also emphasizes the need to include individualized exercise programs (e.g., range-of-movement exercises), as well as patient education and participation in clinical research.
Dr. Matteson emphasizes that most patients with PMR can be managed successfully with modest (i.e., not exceeding 25 mg/day) initial doses of prednisone. “Every effort should be made to reduce the glucocorticoid burden by careful dose reduction and consideration of glucocorticoid-sparing therapy, [which is] currently methotrexate,” he says.

