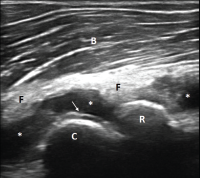
Figure 1. Ultrasound of the left elbow: anterior humero-radial longitudinal view. A large anechoic to hypoechoic collection (*) is present in the anterior elbow joint, which superiorly displaces the fatpad (F) and the brachialis muscle (B). This collection extends proximal to the humeral capitellum (C) into the radial fossa (left sided *) and distal to the radial head (R) to the annual recess (right sided *). There is a hyperechoic linear band (arrow) over the superficial margin of the hyaline cartilage of the humeral capitellum.
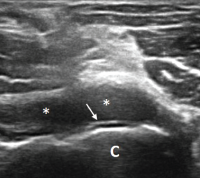
Figure 2. Ultrasound of the left elbow: anterior transverse view of the radial aspect of the joint. A large anechoic collection (*) is present in the anterior radial joint space. There is a hyperechoic linear band (arrow) over the superficial margin of the hyaline cartilage of the humeral capitellum (C).
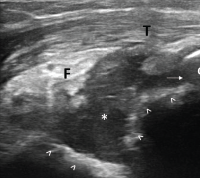
Figure 3. Ultrasound of the left elbow: posterior longitudinal view. There is a large, anechoic to hypoechoic collection deep to the triceps muscle (T) in the olecranon fossa (*) and posterior elbow joint recess (arrow), which superiorly displaces the posterior fatpad (F). For landmarks, note the olecranon process (O), the humeral trochlea (arrows).
Diagnostic Pearls
In this patient’s multidisciplinary evaluation, we bring up two diagnostic pearls.

