click for large version
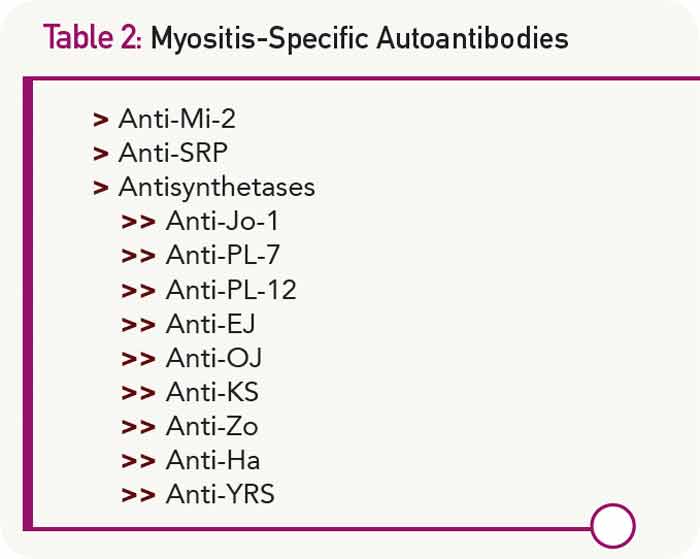
Table 2: Myositis-Specific Autoantibodies
The Differential Diagnosis Is Huge
Another challenge in diagnosing idiopathic inflammatory myopathies involves differentiating them from many other conditions, considered to be myositis mimics, which can also fulfill Bohan and Peter’s criteria (see Table 1). Bohan and Peter recognized the relative nonspecific nature of their criteria, stating, “There are certain findings, herein called exclusions, whose presence should make one very cautious about rendering a diagnosis of polymyositis.”2

