click for large version
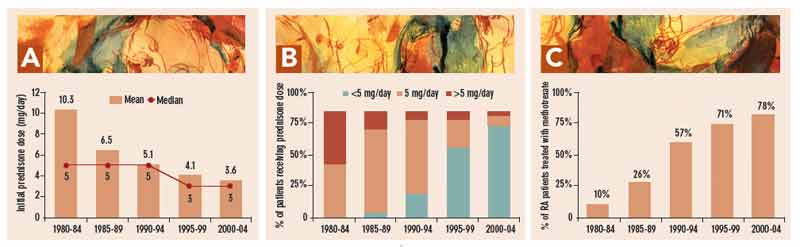
Figure 1: A) Mean and median initial prednisone dose in 308 patients with RA seen between 1980 and 2004, computed in five-year periods: 1980–84, 1985–1999, 1990–1994, 1995–1999, and 2000–2004.25 B) Percentage of patients with RA whose initial prednisone dose was <5, 5, or >5 mg/day in the respective five-year periods.25 C) Percentage of patients with RA who were treated with methotrexate in the respective five-year periods.23
click for large version
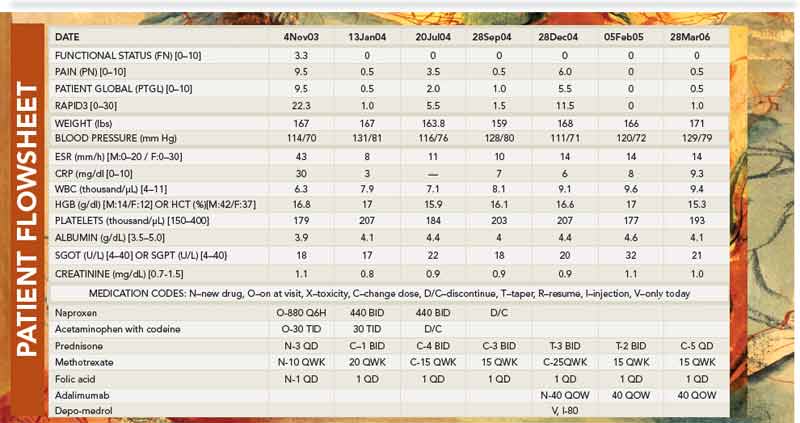
Figure 2: Flowsheet of a man who presented at age 61 with rheumatoid arthritis, with scores for physical function of 3.3, pain 9.5, global status 9.5, and RAPID3 of 22.3 (on 0–30 scale). He was treated with methotrexate 10 mg/week and prednisone 3 mg/day. Two months later on January 13, 2004, his RAPID3 score was 1, indicating a near-remission situation. He did very well for almost a year, as documented for visits on July 20 and September 28, 2004 (RAPID3 score was 5.5 on July 20, but this was due to acute back strain and not inflammation, so therapy was not altered). On December 28, 2004, he presented with a severe flare. His joints were once again swollen, and although his physical function score was 0, pain was 6.0 and global 5.5. He was offered the possibility of an anti–tumor necrosis factor agent, adalimumab, which he elected to receive. Two months later, on February 5, 2005, all his scores were 0, indicating an excellent response. This status was maintained for more than a year, as indicated by his visit of March 28, 2006.
The case for treatment with prednisone in doses of 5 mg/day or less includes:
