Because of these considerations, there should be economic savings in employing a solid-phase immunoassay for quantitating an ANA. Thus, in an attempt to develop solid-phase ANA immunoassays, a number of groups have put onto the solid phase whatever antigens are typically assayed in the more specific ANA immunoassays (e.g., DNA, Sm, RNP, Ro/SSA, La/SSB, nucleoprotein, cell extracts, etc.). In published reports, the correlation coefficient between ANA titers and these solid-phase assays is quite good. Thus, many commercial firms have switched their ANAs to these solid-phase immunoassays.4-23 Of concern, however, is the high frequency/percentage of false-negative results in patients with known SLE and related diseases, as well as the continued high frequency of “false positives” (e.g., a positive ANA in someone without SLE) in these studies.15-21 Further work is needed to improve the sensitivity and especially the specificity of these solid-phase immunoassays to ensure that patients with SLE and related diseases are not missed by these solid-phase immunoassays.
Antibodies to DNA
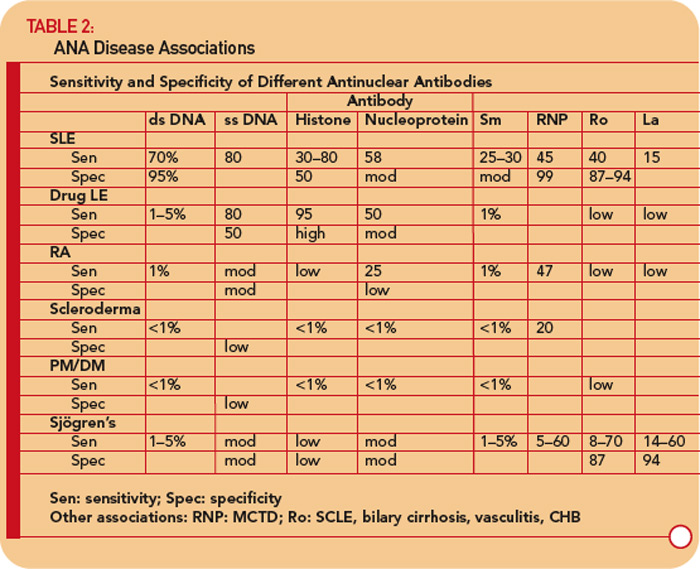
Antibodies to DNA can be primarily divided into those that react with single-stranded (ss) DNA and those recognizing dsDNA.24-26
Anti-ssDNA antibodies have been reported in SLE, rheumatoid arthritis, drug-related lupus, healthy relatives of patients with SLE, and, less commonly, in other rheumatic diseases. (See Table 2, p. 17.) Thus, anti-ssDNA has limited usefulness for the diagnosis of SLE or other rheumatic diseases. Anti-ssDNA does not correlate well with disease activity and are therefore not useful for disease management.