click for large version
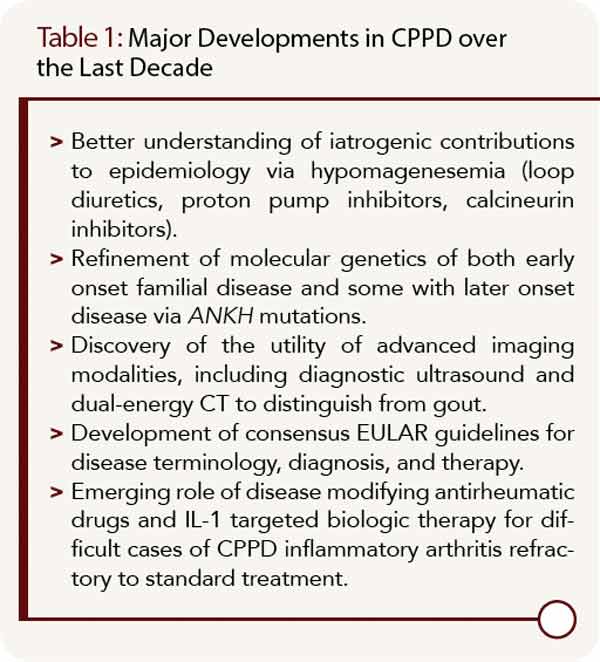
Table 1: Major Developments in CPPD over the Last Decade
Developments in CPPD Epidemiology
In most patients, CPPD appears to represent a systemic articular and soft tissue pathophysiology disorder in aging, a paradigm reinforced by the results of the unique Genetics of Osteoarthritis and Lifestyle study cohort (GOAL).1,2 In GOAL, radiographic evidence of CPPD at one joint was frequently associated with CPPD at distant joints, whether osteoarthritis (OA) was present or not.2 One unexpected nuance of GOAL was that knee OA, but not hip OA, was associated with radiographic evidence of CPPD at distant joints.2

