BLACKDAYutterstock.com
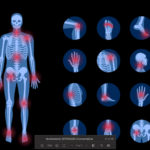
Palindromic rheumatism (PR) was first described in 1944 as “unique in its nature of recurrent, transient episodes of excruciatingly painful inflammation of articular and periarticular tissues, followed by periods without symptoms.”1 Unfortunately, it is becoming evident this entity is more frequent than we thought.2
PR is easily ignored or misdiagnosed due to its character (i.e., no symptoms or signs between attacks) and because patients usually present after resolution of symptoms, with no evidence of acute inflammation on clinical, serologic or radiologic examination.