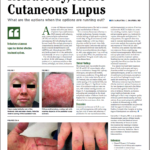
Figure 1: Bullous lesions on the finger extending to the elbow.
Systemic lupus erythematosus (SLE) is a heterogeneous disease associated with multiple acute or chronic cutaneous manifestations, including the relatively rare category of bullous lupus. The development of vesiculo-bullous lesions may be associated with a high morbidity, hence they warrant an urgent investigation, including a skin biopsy to identify the diagnosis and initiate prompt treatment.
With this case, we are going to describe the occurrence of progressive bullous skin lesions in the absence of fever and leukocytosis in a patient with known SLE and discoid lupus on immunosuppressive therapy. This case highlights the importance of considering a broad differential diagnosis as the treatment can be vastly different.
The patient presented to the hospital with generalized malaise, polyarthralgia, alopecia and acute worsening of her chronic skin disease with a flare of her malar rash and discoid lesions on the face, chest, hands and feet. On presentation, she was hemodynamically stable and afebrile. Blood work revealed anemia, lymphopenia with normal liver and renal function and a normal urinalysis. She had reduced complement levels—the C3 was 32.1 mg/dL (normal 83–193 mg/dL), and the C4 was 2.9 mg/dL (normal 15–53 mg/dL)—and an elevated anti-ds-DNA (87 IU/mL) (normal
Given the severity and the extent of her skin lesions, she was started on pulse-dose intravenous steroids. She had responded well to this therapy in the past. High-dose steroids led to resolution of some lesions, but within a few days, new lesions appeared, involving her limbs, abdomen and thighs (see Figure 1), with morphological evolvement of the rash to form painful desquamating bullous lesions filled with serous fluid. The malar rash did involve the naso-labial fold (see Figures 2a, 2b). Nikolsky’s sign was positive. There was also purulent discharge from both eyes, with inflammation of the iris, and bullous lesions were visible on the external ear. Importantly, there was the notable absence of oropharyngeal or vaginal mucosal involvement.

Figures 2a and 2b: Vesiculo-bullous lesions on the face and neck after the patient received steroids on admission.