Bullous lupus is relatively rare—described in 1–8% of patients.4,5 Bullous lupus is caused by the development of antibodies against type VII collagen in the basement membrane and manifests with tense, subepidermal vesiculo-bullous eruptions on an erythematous base, more commonly seen on the trunk, face and upper extremities.5 Immunofluorescence reveals continuous or granular pattern of deposition along the dermo-epidermal junction extending to the dermis.
A 2015 clinic-pathological study described blistering lesions in 22 patients with SLE and, based on their histological description, divided them into three groups.6 One group included five patients with extensive epidermal necrosis appearing as TEN-like lesions. A second group of nine patients had classic cutaneous findings, with interface dermatitis with vacuolization of the basal keratinocytes and lymphocytic infiltrate. The third group of eight patients had neutrophilic bullous lesions.

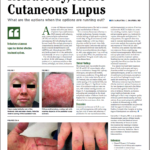
(left) Figure 6: (H&E 60x) Interface vacuolar dermatitis with diffuse acantholysis; note the superficial layer has exfoliated.
(right) Figure 7: Healing lesions after treatment with antibiotics and intravenous immunoglobulins.
SJS and TEN also present as bullous lesions and are dermatological emergencies that usually occur with exposure to new drugs (including disease-modifying anti-rheumatic drugs [DMARDs], such as TNF-alpha inhibitors). However, these conditions usually involve larger body surface area and affect the mucus membranes. Our patient did not have a history of an exposure to a new drug or any other identifiable environmental triggers. She also did not experience any mucosal involvement, making SJS or TENs a less likely possibility.
Studies have described increased morbidity and mortality secondary to infections in SLE patients on immunosuppressive therapy, with a high likelihood of staphylococcal organism involvement due to functional neutrophil dysfunction.7-9 Staphylococcal scalded skin syndrome is caused by an exotoxin released by the bacteria. It attacks the desmosomes, causing detachment of the epidermal layer. It manifests as painful flaccid blisters, positive for Nikolsky’s sign, with widespread desquamation. This disease is more common in children and infants; however, it is associated with mortality rates in adults of approximately 60%, depending on comorbid conditions, degree of immune suppression and delay of treatment initiation.10,11