ARZTSAMUI/shutterstock.com
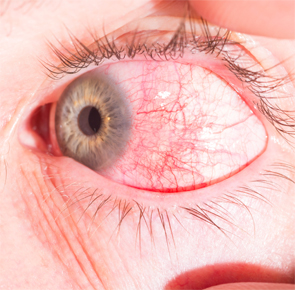
Ophthalmologists may be more likely to initially diagnose and treat scleritis, an inflammation of the scleral tissues of the eye. However, rheumatologists need to remain aware of the condition as well: It’s commonly associated with rheumatic disorders, such as rheumatoid arthritis (RA).
Scleritis can present in the eye anteriorly or posteriorly. “Anterior scleritis can be diffuse, nodular, necrotizing with inflammation and necrotizing without inflammation,” says ophthalmologist Gaston O. Lacayo, III, MD, Center for Excellence in Eyecare, Miami. “The most common clinical forms are diffuse scleritis and nodular scleritis.”

