Third, we must develop an understanding of the “neuro-immune” interface that governs the cortical sensation of dryness or pain.
- Our failures in better managing neuropathic pain become very evident when managing our patients with SS.
- Thus, a better collaboration between rheumatology and other medical specialties, such as neurology, and pain medicine for clinical trials should improve the outlook for the next decade’s therapy.
In a previous issue of The Rheumatologist (November 2013), we described a model of “phantom pain” and how it might play a role in the difference between patients’ symptoms and objective findings.
Background
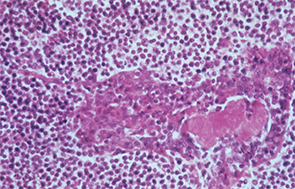
In this patient with Sjögren’s syndrome, most of the parotid gland parenchyma has been replaced by a diffuse collection of lymphocytes, which sometimes leads to an erroneous histologic diagnosis of malignant lymphoma. The lumen of the salivary ductule in the center of the field is occluded by an eosinophilic deposit of inspissated or thickened secretion; the duct lining cells are markedly hyperplastic (epimyoepithelial islands).
Image Credit: Rheumatology image library


