A chest CT (see figures below and on p. 24) demonstrated advanced, Stage IV pulmonary sarcoidosis with significant architectural distortion related to multiple mycetomas visualized in the left upper lobe, right middle lobe and right upper lobe, and markedly distorted bronchiectatic airways connecting to the dominant mycetomas. Pulmonary angiography localized bleeding from both bronchial arteries, as well as a branch of the right bronchial artery, which was supplying the right upper lobe. Interventional radiology performed successful particle embolization of the culprit arteries.
Pulmonary hypertension is commonly seen in Stage IV sarcoidosis, & steroids have not been shown to result in a significant hemodynamic response in this subset of patients. Thus, the role of steroids in advanced stage IV disease is limited.
Laboratory studies were significant for a positive Platelia (ELISA for Aspergillus) of 5.27 (index ≥0.5 is positive) and Fungitell assay greater than 500 pg/mL (glucan values ≥80 pg/mL are positive), confirming aspergillosis. Voriconazole therapy was initiated, and the patient was discharged home with a steroid taper schedule. After further evaluation, he underwent lung transplantation two months later.
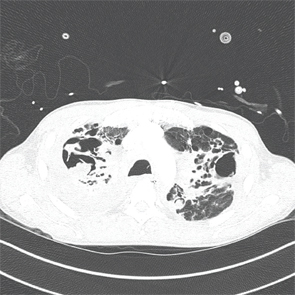
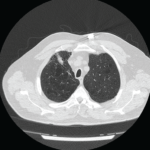
An axial CT view demonstrating a large mycetoma in the right upper lobe and a left upper lobe cavitating lung lesion.
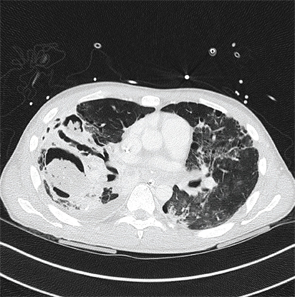
An axial CT view demonstrating a mycetoma in the right lower lobe.
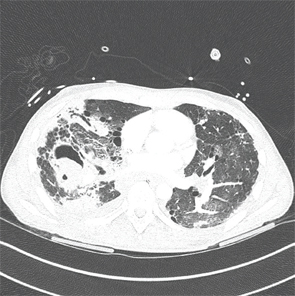
An axial CT view demonstrating a mycetoma in the right middle lobe.
Discussion
Asymptomatic pulmonary sarcoidosis, regardless of stage, does not require the initiation of steroid therapy, but rather should be monitored for clinical progression. Steroids should be considered in patients with significant symptoms (e.g., cough, dyspnea, hemoptysis), worsening radiographic findings and worsening pulmonary function tests.1