Hemoptysis is thought to arise from local vascular invasion by the Aspergillus organism, and it can result in life-threatening bleeding, as seen in this patient. Itraconazole, voriconazole and even intracavitary amphotericin B and voriconazole have been used to treat aspergillomas, but the treatment of these infections in sarcoidosis is not well established.4
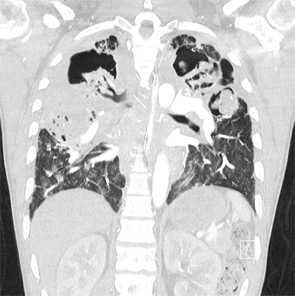
A coronal CT view demonstrating right and left upper lobe mycetomas.
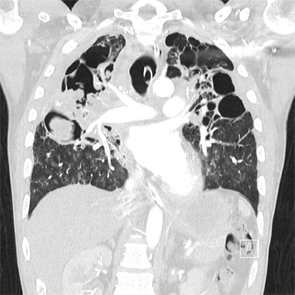
A coronal CT view demonstrating right upper and middle lobe mycetomas.
Conclusion
The potential role and appropriate dosage of corticosteroids should be carefully evaluated in patients with pulmonary sarcoidosis. These patients should be monitored for changes in symptoms, including worsening cough, hemoptysis and dyspnea, because these may imply worsening sarcoidosis, but they should also be evaluated thoroughly to rule out infection, malignancy or worsening pulmonary hypertension. Steroids carry significant and potentially life-threatening risks and are not warranted in all patients with this disease.