WASHINGTON, D.C.–Interstitial lung disease (ILD) is associated with a number of rheumatic diseases, and patients may be referred by pulmonologists to rheumatologists for management. Patients with one of these conditions, especially when associated with connective tissue diseases, often have poor prognoses. Diagnosis can be challenging, and there are still few effective therapies for many of these conditions.
A panel of experts on connective tissue–associated ILD spoke at a session titled, “Connective Tissue Disease–Associated Interstitial Lung Disease,” at the 2012 ACR/ARHP Annual Meeting, held here November 9–14. [Editor’s Note: This session was recorded and is available via ACR SessionSelect.] They offered some insight on diagnosing and treating these patients, as well as a glimpse into areas of research that may be promising.
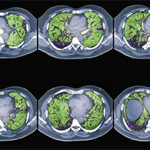
ILD is a group of conditions associated with many connective-tissue diseases, said Aryeh Fischer, MD, acting chief of the division of rheumatology at National Jewish Health in Denver. These conditions typically are marked by interstitial inflammation and/or fibrosis of the lungs. Symptoms are not always clear, but imaging, histopathologic, and function tests may provide the best clues for diagnosis, he said.
Serious and More Mild ILDs
One of the most serious connective tissue–associated ILDs is usual interstitial pneumonia (UIP), an idiopathic condition marked by a honeycombing pattern seen on radiographs and fibrosis, Dr. Fischer said. UIP is most commonly seen in rheumatoid arthritis (RA) and is also commonly seen in scleroderma and systemic sclerosis. It has the worst prognosis in this classification, Dr. Fischer noted.
Another commonly seen ILD in rheumatic diseases is nonspecific interstitial pneumonia, a condition with a better prognosis than UIP. Prognosis for survival can depend on factors like the patient’s age, smoking status, and familial history, Dr. Fischer noted. Patients with RA may also develop bronchiolitis obliterans organizing pneumonia, an inflammation of the bronchioles with a comparatively good prognosis for recovery. Other conditions that may be seen in rheumatic disease patients include lymphocytic interstitial pneumonia and, more rarely, severe acute interstitial pneumonia.
Where ILD Is Most Common
ILD is most commonly found in systemic sclerosis at a prevalence rate of 25% to 90%, Dr. Fischer said. It is also found less frequently in polymyositis and dermatomyositis, RA, Sjögren’s syndrome, and systemic lupus erythematosus. If rheumatologists are treating patients with known connective tissue disease, they should take steps to determine if possible ILD is connective tissue disease¬ associated, Dr. Fischer said. Recognition of the exact disease would affect treatment decisions and the prognosis for these patients. “It’s important for the patients’ outcome to see where they fit,” he said.