click for large version
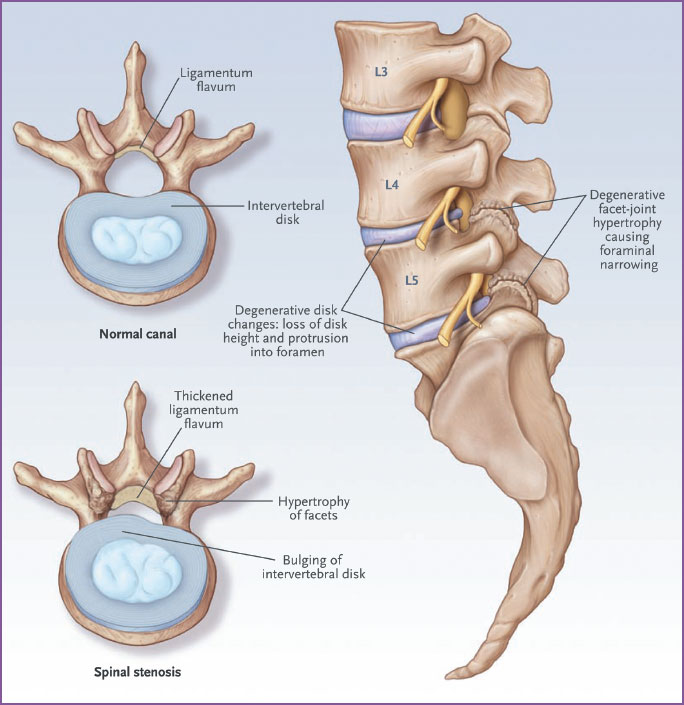
Figure 1. Pathoanatomical features of degenerative lumbar spinal stenosis. The axial view in the upper left shows a cross-section of a normal lower lumbar spine. The axial view in the lower left shows a cross-section of the lumbar spine with features that are consistent with lumbar spinal stenosis, including bulging of the intervertebral disc, thickening of the ligamentum flavum, and hypertrophy of the facet joints. The sagittal view on the right shows loss of disc height, disc protrusion, and facet-joint osteoarthritis, all leading to foraminal stenosis. From Katz 2008; copyright Massachusetts Medical Society 2008. Reprinted with permission.
Potential Solutions to These Diagnostic Challenges
It is important for clinicians to listen and examine carefully, and to form an impression based on the history of physical examination findings, the patient’s age, and other such clues. If the clinician senses that spinal stenosis is reasonably likely on the basis of several history and physical examination findings, imaging tests can be useful in confirming the diagnosis. On the other hand, when the clinical picture is not compelling, imaging tests are much less valuable because positive tests are frequently misleading. If imaging tests are performed under similar circumstances, a positive imaging test (or a single positive element of the history or physical examination, for that matter) can often be disregarded.