
Figure 2: DECT of hands #1
Pegloticase is a new alternative therapy for patients with severe, refractory gout unresponsive to other urate-lowering agents. The goal of this therapy is to reduce disease burden, tophi size and frequency of flares and to improve quality of life when other treatments have failed. Persistent lowering of plasma uric acid (PUA) to less than 6 mg/dL, while achieving the therapy’s goal, is considered successful treatment.
Prior studies have shown that although all patients initially respond to pegloticase, as indicated by decreased PUA levels, not all patients maintain that response. The reasons are multifactorial, but as research has progressed, several studies have shown that gout can be heritable, and both genetics and antibody formation to drug therapy can affect both overall disease and response to treatment.
Herein, we present a case of severe refractory gout in a patient unresponsive to all standard urate-lowering therapies, as well as treatment with pegloticase.
Case Description
A 65-year-old African American male with a past medical history of stage II chronic kidney disease and hypertension was referred to our clinic for poorly controlled, erosive, polyarticular gout. The patient was first diagnosed at the age of 45 with initial joint involvement noted only in the right knee and left wrist. Over time, he had gradual progression of his disease, with involvement of his hands, wrists, elbows, knees, ankles and feet, as well as development of multiple tophi over his extremities. Moreover, he had experienced numerous flares over the course of his disease, averaging approximately six each year.
(click for larger image)
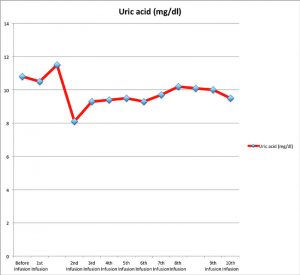
Figure 1: Uric acid (mg/dL) variation prior to and at the time of each pegloticase infusion
At the age of 55, 10 years after the onset of his gout, he required bilateral total knee replacements due to the severity of his disease. Over the past five years, he has had multiple tophi removed from his distal interphalangeal joints (DIPs), elbows and ankles in an effort to improve his overall function. Unfortunately, tophi reaccumulated after each procedure.
At the time of his initial visit to our clinic, he had already failed multiple treatments with non-steroidal anti-inflammatory drugs, colchicine, probenecid, allopurinol and several rounds of prednisone. Given his severe condition, the patient had a significantly decreased quality of life, because he was disabled by the extent of his disease.
Physical examination revealed multiple tophi over his right ear pinna, right third metacarpophalangeal (MCP), right fifth proximal interphalangeal (PIP), left third and fourth DIP, bilateral elbows, bilateral ankles and left foot involving the second and third metatarsophalangeal (MTP) joints. Range of motion was severely limited due to the presence of his numerous tophi.


