click for large version
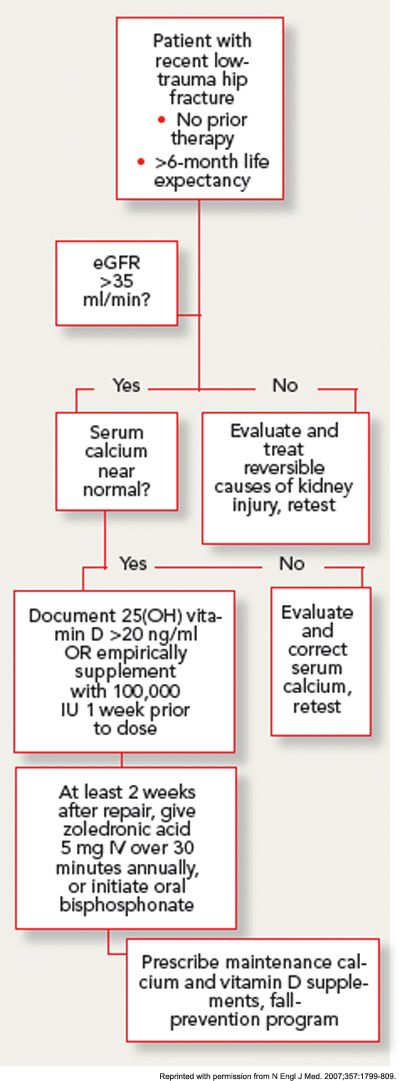
Figure 2: Suggested algorithm for initiating bisphosphonate after low-trauma hip fracture.
With this approach, no clinically significant cases of hypocalcemia were observed, and laboratory-detected hypocalcemia was quite rare and similar in both groups. No cases of vitamin D toxicity were found. Thus, for patients with normal calcium levels, an approach of universal repletion prior to bisphosphonate initiation appears safe. However, it is prudent to await further test results in patients with abnormal corrected serum calcium levels. While the serum levels of 25(OH) vitamin D at which bisphosphonates are safe has not been clearly determined in clinical studies, expert opinion holds that patients with serum levels above 20 ng/mL are unlikely to develop significant hypocalcemia.


