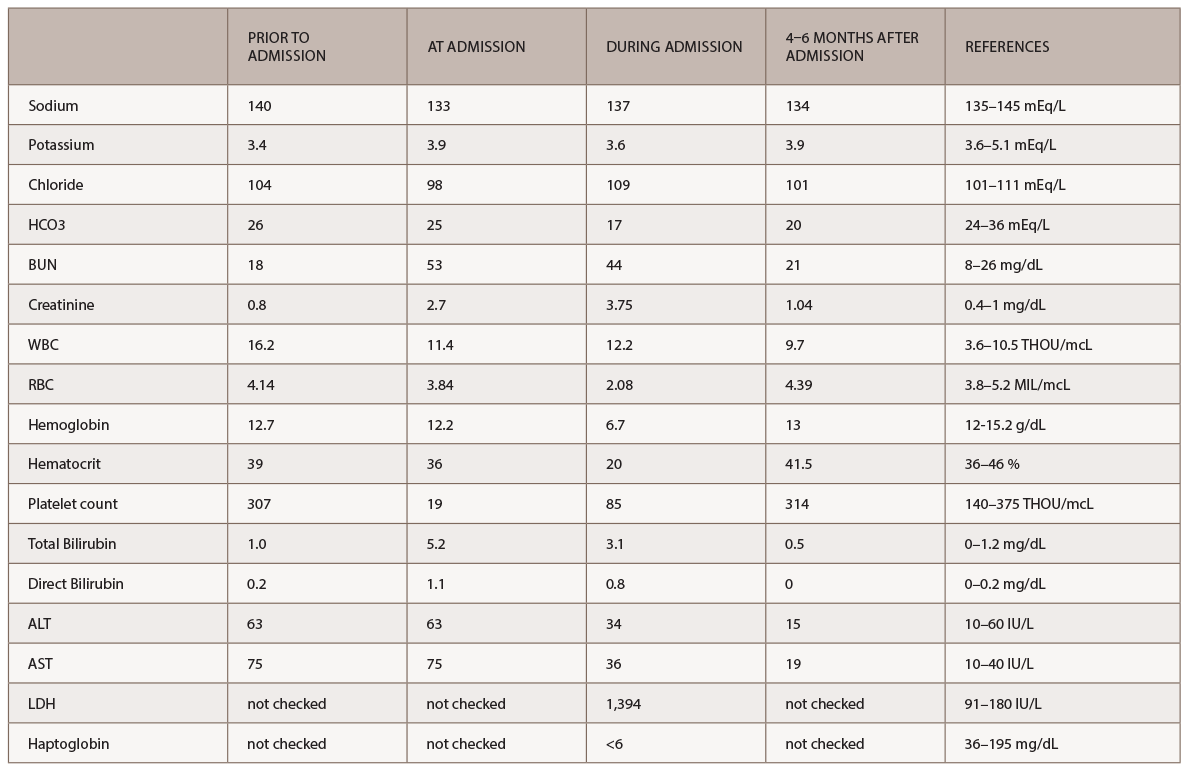
(click for larger image) Table 1: Labs
A new battery of autoimmune tests (see Table 2) was obtained and showed only positive ANA (1:160 speckled). Anti-Scl70, anticentromere, anti-RNA polymerase III, anti-Th/To and anti-U1RNP were all negative. This time, SSA, SSB, anti-Sm and anti-dsDNA antibodies were negative. Complement levels were within normal limits. A CT of the chest demonstrated nonspecific interstitial pneumonia (NSIP) and small bilateral pleural effusions.
Based on the clinical exam findings—specifically, the extensive skin thickening of the face, chest, and upper and lower extremities—the rheumatology team noted this patient satisfied the 2012 ACR classification criteria for definite diagnosis of diffuse systemic sclerosis. Because of the patient’s recent exposure to high-dose steroids and rapid deterioration of renal function, despite a normal blood pressure, the rheumatology consult service suspected SRC.
Per the consulting nephrologist’s request, a kidney biopsy was performed. Renal pathology demonstrated onion skin proliferation within the walls of the intrarenal arteries and arterioles, fibrinoid necrosis and glomerular shrinkage.
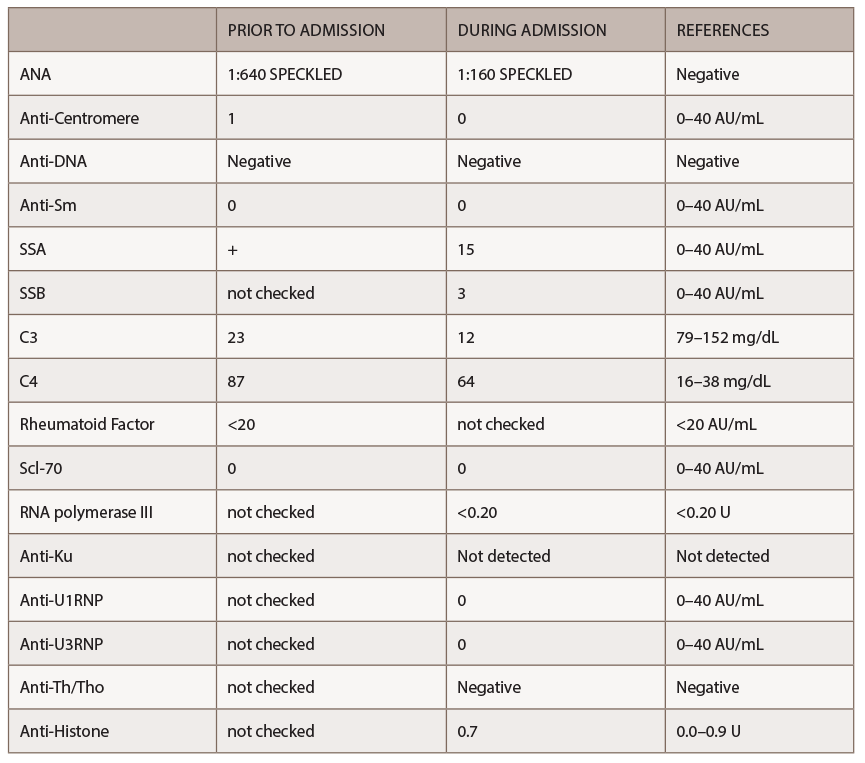
(click for larger image) Table 2: Autoimmune Labs
Based on these findings, a diagnosis of SRC was made. Plasma exchange was stopped, and captopril was initiated. After captopril was started, the patient’s serum creatinine started to stabilize at a value of 3.3 mg/dL.


