For scoring, the weights applied are 0–1 (i.e., 0 is not tender, 1 is tender) for the basic Leeds index, and 0–3 (i.e., 0 has no tenderness and 1–3 indicates increasingly higher degrees of tenderness) for the initial index. The Leeds index counts only acute dactylitis.
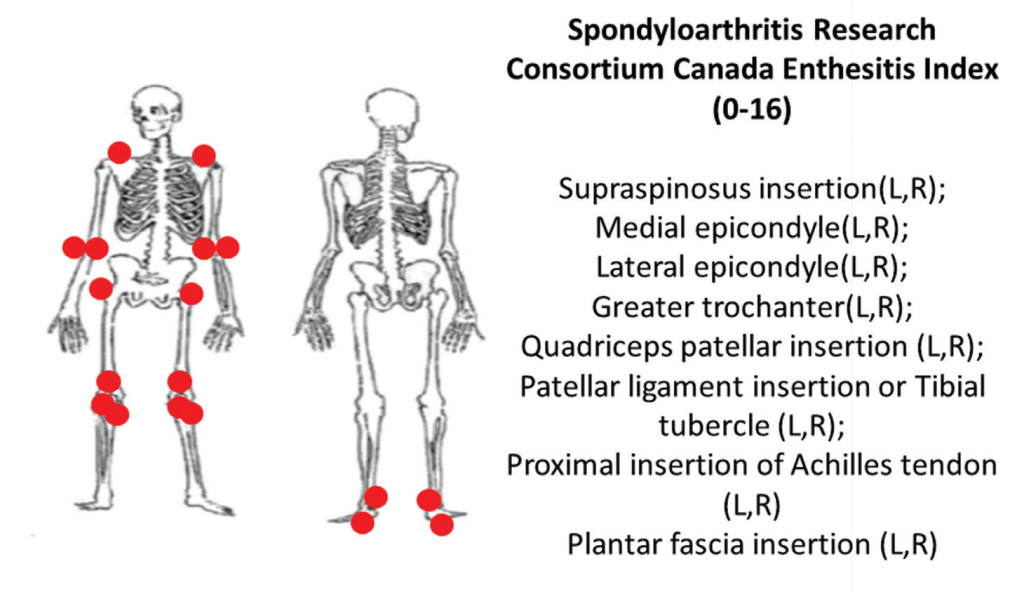
6A: The Spondyloarthritis Research Consortium of Canada clinical enthesitis index.
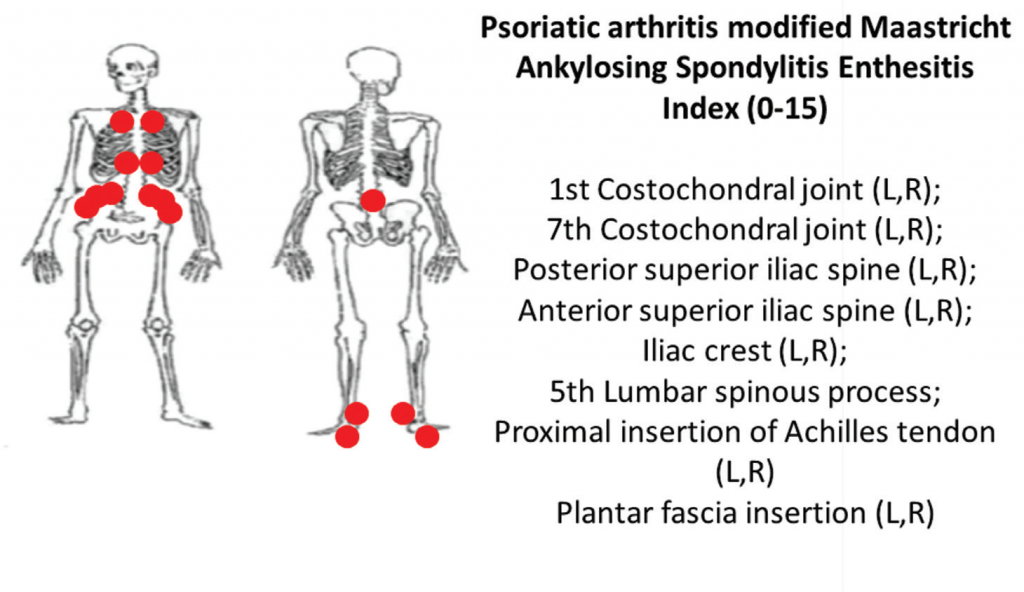
6B: The PsA-modified Maastricht Ankylosing Spondylitis clinical enthesitis index (PsA MASES).z


